
Development of artificial intelligence technology in diagnosis,treatment,and prognosis of colorectal cancer
2022-01-25 02:55:26FengLiangShuWangKaiZhangTongJunLiuJianNanLi
INTRODUCTION
With the invention of the computer,heavy scientific and engineering calculations have shifted from being done primarily by the human brain to being done more quickly and accurately by computers.Artificial intelligence (AI) has evolved rapidly with the continuous development of computer science and technology.AI is an umbrella term that helps humans perform tasks including computer simulation,decision-making,language understanding,problem-solving,voice and image recognition,and other“intelligent” tasks[1-3].AI can be divided into machine learning (ML),deep learning(DL),anti-learning,quasi-supervised learning (QSL),and active learning (AL)[4-7].ML is a subset of AI algorithm which uses statistical techniques to adjust and improve itself[1,3].ML produces algorithms for analyzing data and learning to predict models,which means that ML is data-driven,with a little human intervention as possible in the decision-making process[4,8].The model created by ML can be used as an independent executable system to predict the clinical phenotype[9].The relevant technologies in ML include support vector machine (SVM),neural network (NN),random forest (RF),decision tree,and regression analysis[10].Based on the association of class labels,ML is generally divided into supervised learning,unsupervised learning,and semi-supervised learning (SSL)[8,9].Supervised learning is mainly used for solving classification and regression problems.Unsupervised learning is used for a cluster,density estimation,and dimensionality reduction[9].SSL can significantly improve the learning accuracy when unlabeled data combined with a limited number of labeled data are used in SSL[11].At present,supervised learning plays a leading role in AI and ML in the medical field[2].Supervised learning provides more accurate results than other AI techniques because it considers the characteristics of the patients[10].
Perhaps one of the enduring elements of the Cinderella story comes from the politics of a family, usually a blended family. While many fairy tales have outside antagonists50, Cinderella s trials are in her home and immediate23 family. Return to place in story.
DL is a kind of developed ML based on an artificial NN (ANN)[2],which is inspired by the biological characteristics of the human brain,especially the connection of neurons[2,4].DL can not only automatically find lesions,make recommendations for differential diagnosis,and write elementary medical reports,but can also be selflearning,
,key characters and quantities can be extracted without a manual indication if the training data is provided[4].Moreover,DL aims to copy the brain's learning process and process a large amount of high-dimensional data[12].QSL is a statistical learning algorithm that avoids the manual marking of normal tissue and cancer tissue samples in traditional supervised learning and greatly reduces the intervention of experts[5].ML usually needs a large number of annotated training sets,which are expensive to create.AI reduces the size of the required annotation set and generates a better classification model[7].In some research,to predict the stage of colorectal cancer (CRC) from immune attributes,the anti-learning method has better performance than a series of ML algorithms[6].
Folklore heros, and occasionally heroines, are often given quests and/or tasks to achieve a reward. Here the heroine must search for her husband to prove her worthiness104 and dedication105 after her indiscretion. The most famous quest in folklore is perhaps that of King Arthur s knights106 and their search for the Holy Grail.Return to place in story.
CRC is the second reason for cancer death in males and the third reason for cancer death in females[13].If colonic polyps,which may lead to at least 80%-95% of CRC[14],are detected by the screening procedure and resected in the precancerous stage,it can help prevent CRC development[15].Although early and intensive screening can reduce cancer incidence and mortality,patients avoid CRC screening due to the complexity and cost of screening[15-17].Generally,the methods of diagnosing CRC are divided into imaging diagnosis,endoscopy,and pathology diagnosis.Treatment methods are divided into endoscopic treatment,surgical treatment,and drug treatment.If lymph node metastasis is not confirmed preoperatively,lymph node dissection is not required intraoperatively[18].AI has great diagnostic potential because it can learn from a large data set.In the clinical image,AI is superior to medical experts and existing biomarkers[10].This paper will describe the use of AI in the diagnosis,treatment,and prognosis of CRC.Web of Science and PubMed databases were searched using keywords “artificial intelligence” and “colorectal cancer”.
USE OF AI IN DIAGNOSIS OF CRC
DL in imaging diagnosis
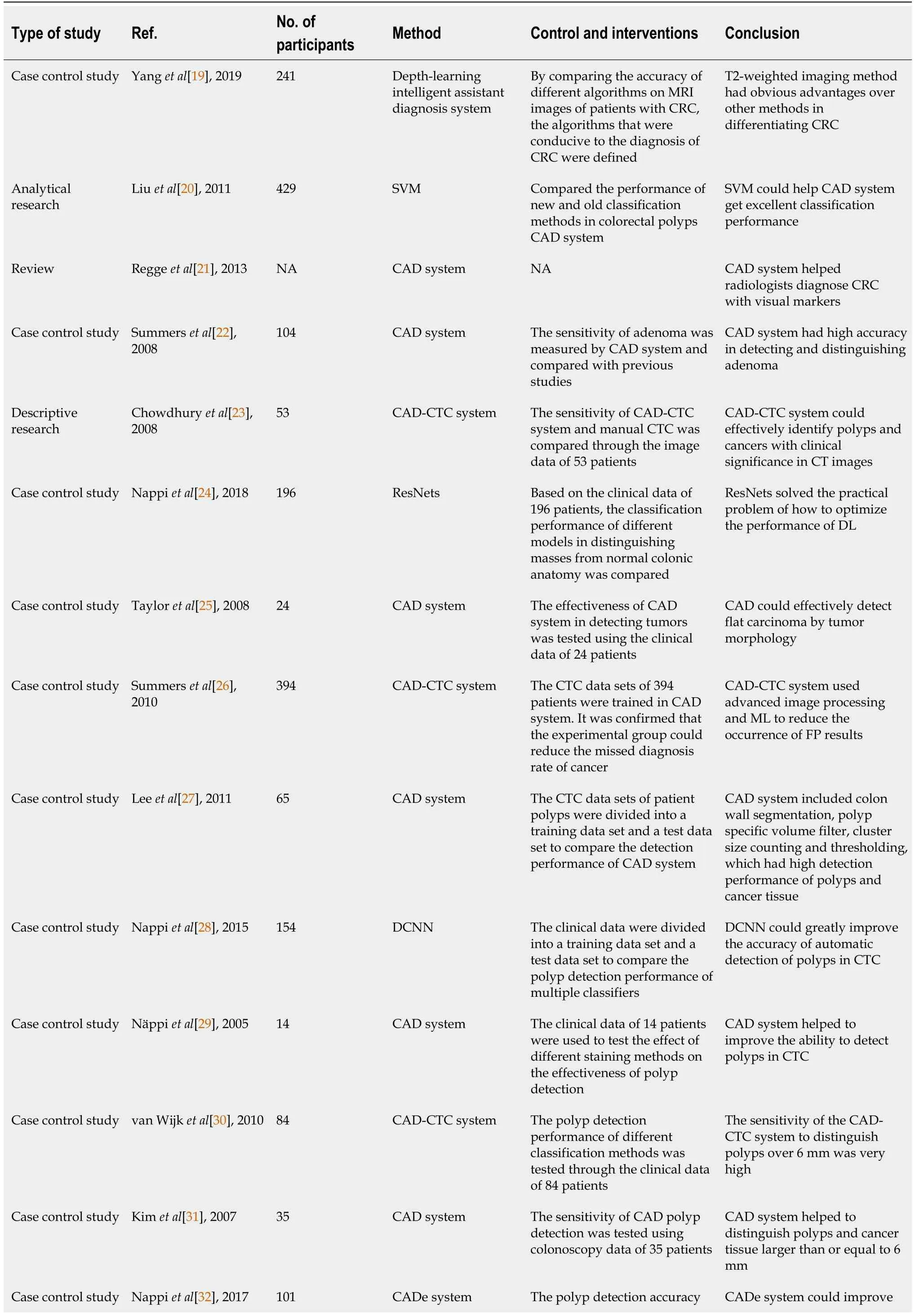
The DL intelligent assistant diagnosis system can help the clinical diagnosis and treatment of CRC[19].The computer-aided diagnosis (CAD) system usually analyzes the nature of the selected area (cancerous or noncancerous) through the informative characteristics of the known potential (cancerous) structure[20].The CAD system can help radiologists diagnose CRC by visual cues (CAD marks) associated with potential pathology.In addition,CAD can help determine the location of the disease (computeraided detection,CADe) and determine whether the abnormality is benign or malignant.Regardless of the outcome,doctors must ultimately decide whether to“believe” the CAD mark[21].The key for radiologists accepting the clinical use of CAD systems is to have a high detection sensitivity and a low false-positive rate (FP)[20].Apart from polyps and cancer,other colorectal pathological morphologies are rare,which can explain why CAD solutions for computed tomography colonography (CTC)have developed so rapidly[22].CAD of CTC has indeed improved sensitivity in finding polyps without disproportionately decreasing specificity,but the lesions mistaken for false-negative are significantly large and irregular[21-23].Regge
[21]believed that the difficulty of characterization (irregular and flat morphology) was the main determinant of radiologists’ rejection of true positive CAD indications.
Then he turned round sharply, and, seizing the little creature by his beard, he gave him such a shaking that he tore his beard out, and the dwarf sank groaning19 to the ground
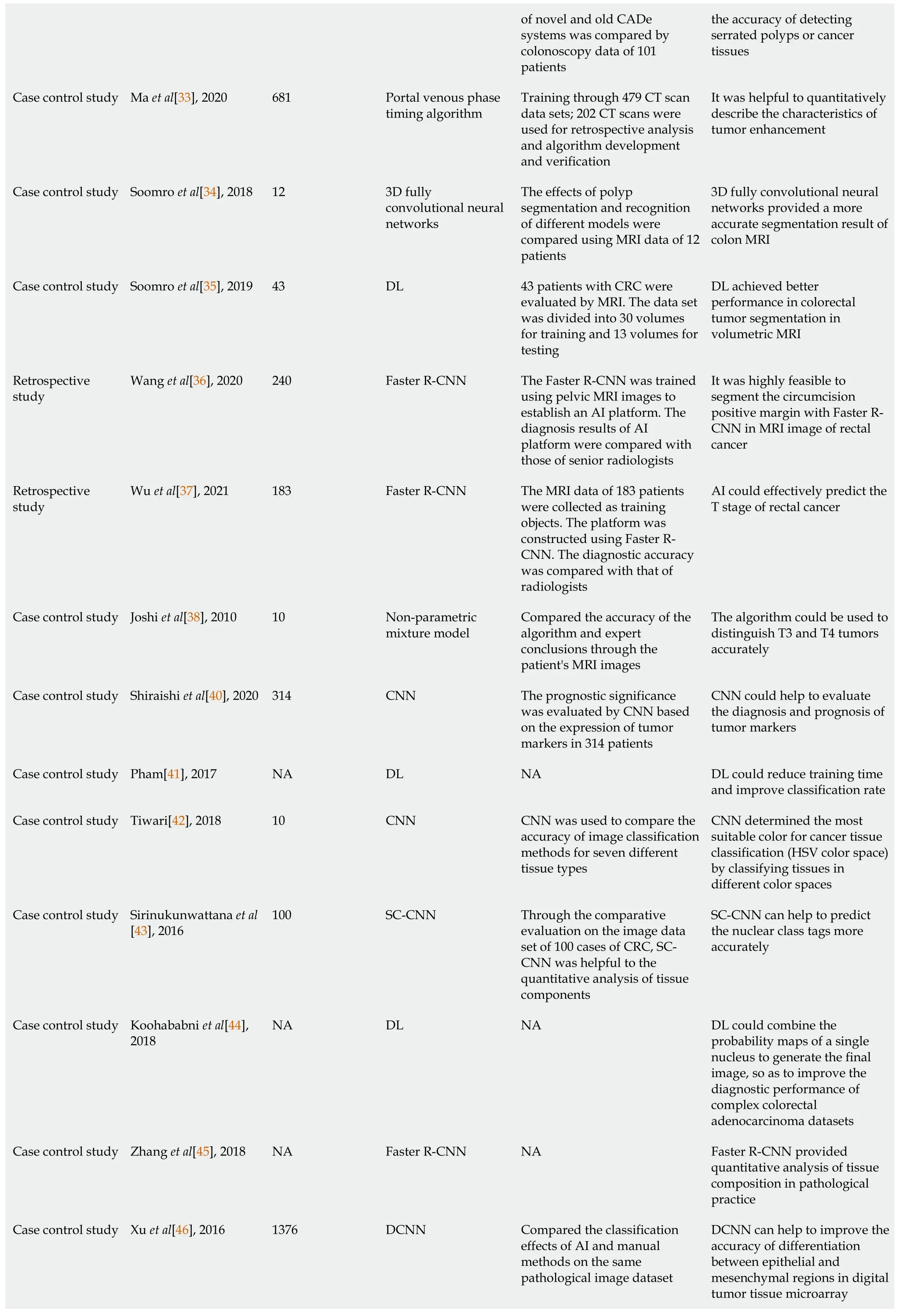
The optimal portal venous phase timing recognition scan was selected for classifying the contrast enhancement time,which could help analyze the radiologic characteristics of the tumor and evaluate the efficacy of patients with advanced CRC[33].Soomro
[34] found that three-dimensional (3D) fully convolutional NNs combined with 3D level-set showed a higher sensitivity than 3D fully convolutional NNs alone in the segmentation of CRC on magnetic resonance imaging (MRI),which helped for the diagnosis of CRC.In 3D-T2 weighted MRI,the 3D full collaborative network architecture based on DL could segment CRC more reasonably and effectively than other techniques[35].In the high-resolution MRI image of rectal cancer,the use of a faster region-based convolution NN (Faster R-CNN) had a high accuracy in evaluating tumor boundaries[36,37].Circumferential resection margin is one of the key factors affecting the treatment decision of CRC patients.Joshi
[38]proposed an automatic calculation and visualization method of circumferential resection margin distance in MRI images of CRC to segment the middle rectal fascia,the corresponding tumor,and lymph node into different regions.The segmentation was used to analyze the shortest cut edge automatically,and the results obtained were almost identical to the experts’ judgment[38].
DL in pathological diagnosis
As one of the most common cancers globally,CRC is a result of multi-step and multifactor action.The key to early diagnosis and improving the overall survival rate is determining the high-risk population[128].Some related risk factors may increase the possibility of CRC,such as age,lifestyle,personal disease history,and genetic syndrome[129].In order to establish a risk prediction model of CRC,appropriate feature selection is needed.It is important to identify features with predictive power for taking appropriate interventions to address risks[130].Each AI technology generates different important attributes to evaluate tumor prognosis based on potential biases and assumptions.Based on the accuracy and the minimum deviation,it is clear that the most significant tumor characteristics are lymphocyte infiltration,Dukes stage,age,and mitotic count[131].Tumor invasiveness score is a new prognostic factor for predicting tumor stage in colon cancer patients[132].It helps use ML to increase patient ethnicity in cancer survivability prediction and support personalized general medicine[133].Most medical studies concentrate on treatment and etiology rather than prediction because prediction tends to be uncertain and risky.The decision tree classifier can predict recurrence or death according to various factors.It is beneficial for doctors to make further treatment decisions and avoid unnecessary treatments[134].An accurate prognosis is a basis of making an appropriate treatment plan for cancer patients.Because of the heterogeneity of the disease and the inherent limitations of the pathological reporting system,the outcomes are very different for patients in similar stages of pathology.ML used different types of features that could be easily collected from immunofluorescence images to predict phase II mortality,and ML had more accuracy than current clinical guidelines[135].
Convolutional NN (CNN) is a common method in pathological image analysis.Compared with other methods,CNN has the advantages of convenience for end-toend learning (CNN learning parameters and representations are designed manually),flexibility,and high capacity[2].The choice of color space is important for identifying cancer tissue because it deeply affects the performance of the classification model.CNN is used to analyze the tissue classification of different color spaces.Tiwari S proved that hue,saturation,value (HSV) color space was more suitable than any other color model for cancer tissue classification[42].Because of the heterogeneity of the cells,texture,and cell contact complexity,it is challenging to detect and classify the nuclei in the pathological images of cancer tissues stained with hematoxylin and eosin(H&E)[43,44].A space-constrained CNN based on DL was proposed for nuclear detection,which might provide a possibility for quantitative analysis of tissue components and clarify the tumor microenvironment.Moreover,the neighbor ensemble predictor combined with CNN could accurately predict the detected nuclear markers and classify the nuclei[43].Although qualitative and quantitative analysis of histopathological images can clarify the tumor and explore various options for cancer treatment,it remains challenging due to cell heterogeneity.Zhang
[45] proved that it had a good accuracy and lower cost of time when Faster R-CNN was used in feature extraction,providing a useful quantitative analysis group for pathological practice.
CNN,widely used to analyze histopathological images,only performs directly on the histopathological images,ignoring the histopathological images’ stain decomposition.Xu
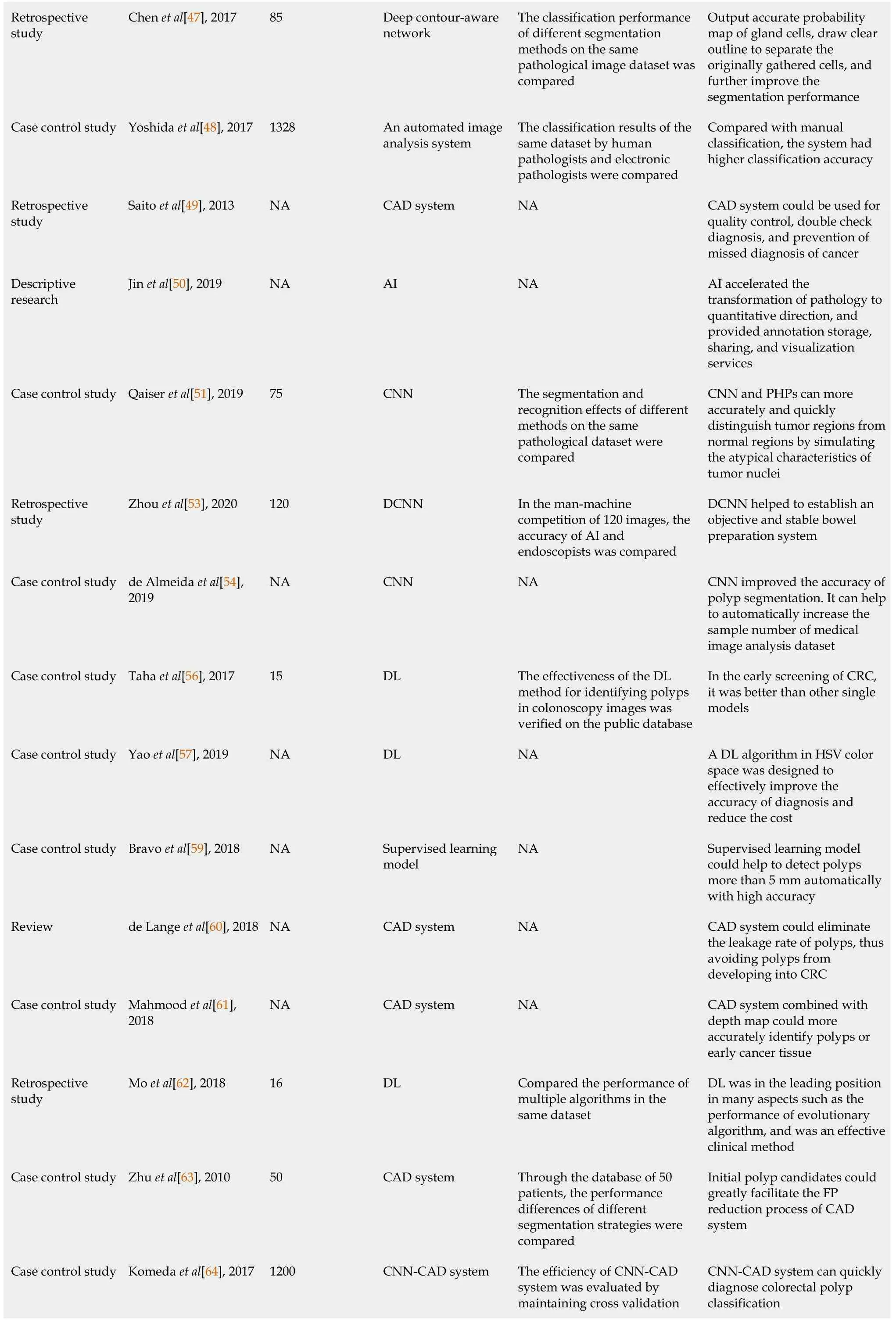
[46] reported a new model based on DCNN to classify the H&E and immunohistochemistry images of epithelial and stromal cells in colon cancer.For distinguishing stromal from epithelial cells,the DCNN based model was always better than the traditional hand-made model.The morphology of glands and nuclei is used to evaluate the malignant degree of adenocarcinoma.As a necessity for quantitative diagnosis,the accurate detection and segmentation of the histological image are challenging due to its appearance variation,strong similarity,and tissue degradation.Chen
[47] attempted to use a depth profile awareness network,which could output the accurate probability map of histological objects and draw clear contour lines,to improve the accuracy of detection and segmentation.
Digital pathology is a new field.The development of digital pathology may help pathologists to improve the quality of routine pathological operations[48].The key to promoting the development of digital pathology is the CAD system,based on the principle of extracting histopathological features that pathologists consider important.Then,the existence of these features was explained quantitatively by computer calculation[49,50].There are two important steps towards the CAD:Tumor segmentation of the whole section image in the histological section and the automatic segmentation of tumors in the H&E staining histological image[51].Qaiser
[51]found that tumor and non-tumor plaques had distinct homology,and proved the robustness and significance of persistent homology by exploring connectivity between nucleus.A method called persistent homology maps (PHPs) was proposed,which could distinguish tumor area from the normal area by simulating the atypical characteristics of tumor cell nucleus[51].PHPs outperform other methods,including traditional CNN[51].Two different tumor segmentation methods are proposed:Targeting speed without affecting accuracy and targeting higher accuracy.The combination of PHPs and CNN features was shown to be better than competition algorithms[51].
DL in endoscopic diagnosis
Colonoscopy is a common method to screen polyps.The detection and removing of adenomatous polyps can reduce the incidence and mortality rates of CRC [13].AI is necessary to improve machine performance and diagnosis accuracy,reducing the variability between operators and helping rapid treatment decision-making[3].In addition,AI has a great potential to improve the detection rate of adenoma and reduce the cost of polypectomy[52].The quality of intestinal preparation is an important factor influencing the effect of colonoscopy examination[53].When the fecal residues are present in the colon,the rate of missed diagnosis of polyps will increase.Although the endoscopic image diagnostic program based on CNN has yielded good results,its diagnostic ability depends heavily on the quality and quantity of training data[4,54].The use of CNN and colonoscopy procedure is expected to improve the detection rate and diagnosis accuracy of polyps[55].Zhou
[53] developed a CNN based system that was trained by collecting colonoscopy images.Through a human-machine competition,the system was found to be more reliable than endoscopic physicians in diagnosis of CRC.Taha
[56] introduced a DL solution for polyps from colonoscopy,a pre-training architecture for feature extraction,used together with the classical SVM classifier.As the solution can avoid the high computational complexity and high resource requirements of CNN,it outperforms other models in the early screening of CRC[56].Yao
[57] proved that the features in red,green,blue (RGB)and HSV color space could well describe the frames in colonoscopy videos.It could improve the model’s efficiency by integrating the prior knowledge based on vision into the data extracted by DL.Therefore,a feature extraction algorithm in HSV color space was designed to effectively improve the accuracy of diagnosis and reduce the cost[57].McNeil
[58] proposed an automatic quality control system based on DCNN,improving colonoscopy quality by cleaning the mucosal wall and reexamining the rushed segment.The system could increase the detection rate of polyps and have great significance for the early diagnosis and prevention of CRC.
The missed diagnosis rate of traditional colonoscopy approaches 25%[59,60],partly due to the lack of depth information,inter-observer variation,and contrast on the surface of the colon[60,61].Computer-aided technology is important for polyp detection in endoscopic video.The method based on DL takes the lead in the evolution of algorithm performance[62].It is a challenging task for CAD to minimize the FP of colonic polyps[63].Mahmood
[61] used a joint depth learning and graphics modelbased framework to estimate depth from endoscopic images.At the same time,they used the texture-free colon model to generate training images and trained the model with those images[61].The system could estimate the depth of virtual data with a relative error of 0.164,which was helpful to perfect the CAD system and identify lesions[61].Komeda
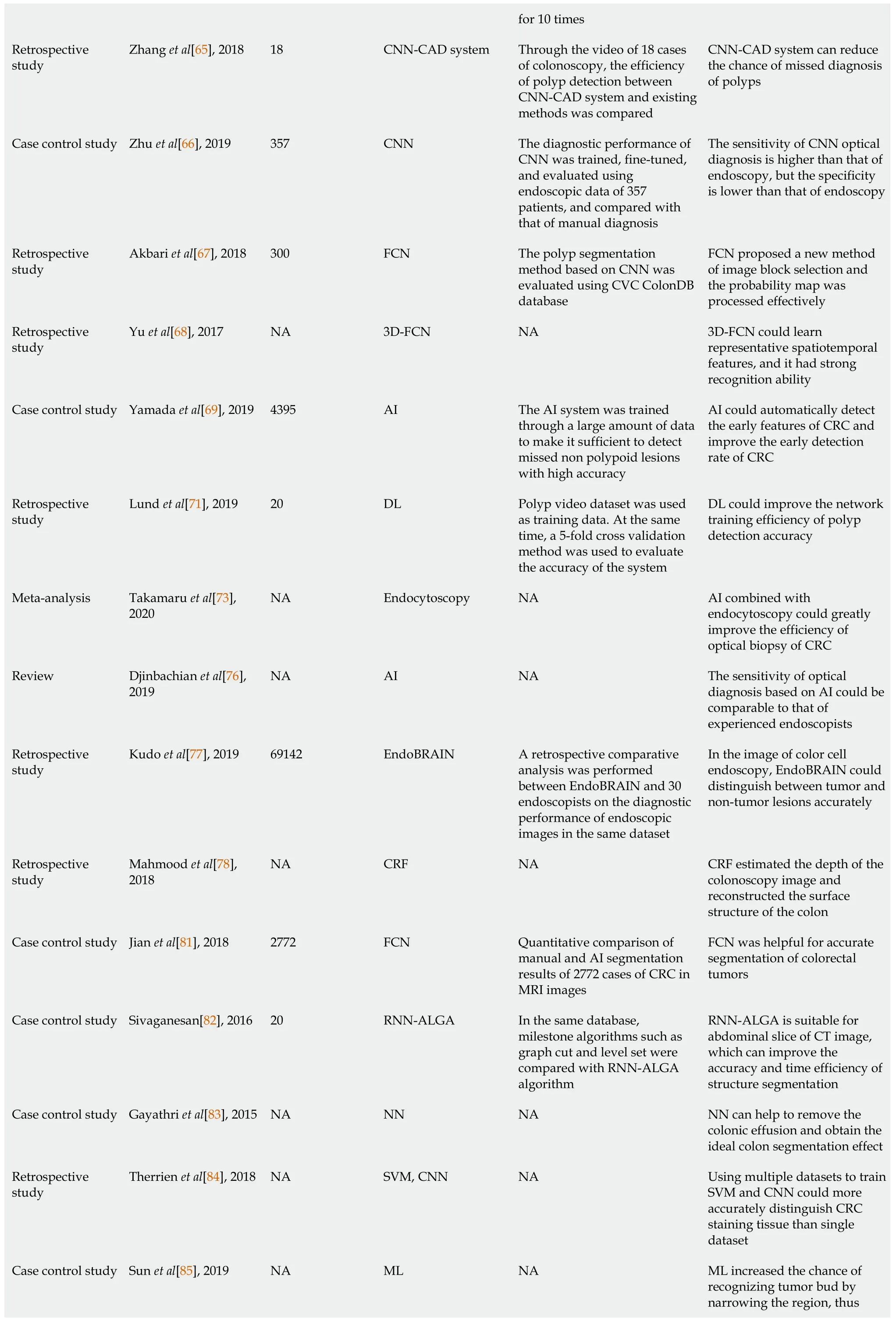
[64] believed that CNN had the advantage of learning from large data and led to high precision and fast processing time,and they designed a CNN-CAD system to study endoscopic images extracted from colonoscopy[64].The analysis and cross-validation of 1200 cases of colonoscopy confirmed that the CNNCAD system was helpful for the rapid diagnosis of colonic polyps and could simplify the decision-making process of colorectal polypectomy[64].Compared with other algorithms,the CAD method (named RYCO) had the potential for rapid and accurate computer-aided polyp detection in colonoscopy.The fast target detection algorithm ResYOLO was pre-trained using a large non-medical image database,and the colonoscopy image was fine-tuned.At the same time,the time information was combined by a tracker named Efficient Convolution Operator to improve the detection results given by ResYOLO.RYCO could clarify the spatial characteristics of colorectal polyps directly and improve the detection efficiency of colorectal polyps[65].In order to distinguish stage T1b and Tis/T1a CRC,the optical diagnostic system developed by CNN was proposed[66].Zhu
[66] selected the early CRC digital images without magnification and under a pure white light endoscope as the training dataset.At the end of the training process,122 early CRC images were used to evaluate the diagnostic performance.The results showed that optical diagnoses by CNN had a high sensitivity but low specificity,which was different from humans[66].Variations in polyp size and shape made the diagnosis of polyp in colonoscopy video challenging[67].However,the Faster R-CNN could reduce the risk of polyp loss during colonoscopy[62].Furthermore,Akbari
[67] presented a fully convolutional network (FCN) method of polyp segmentation based on CNN.In the test phase,they did effective postprocessing for the probability map generated by the network.The CVC-ColonDB database was used to evaluate the method.The result showed that FCN could get more accurate segmentation results[67].3D-FCN could learn more representative spatiotemporal features from colonoscopy video and had stronger recognition ability than FCN[68].
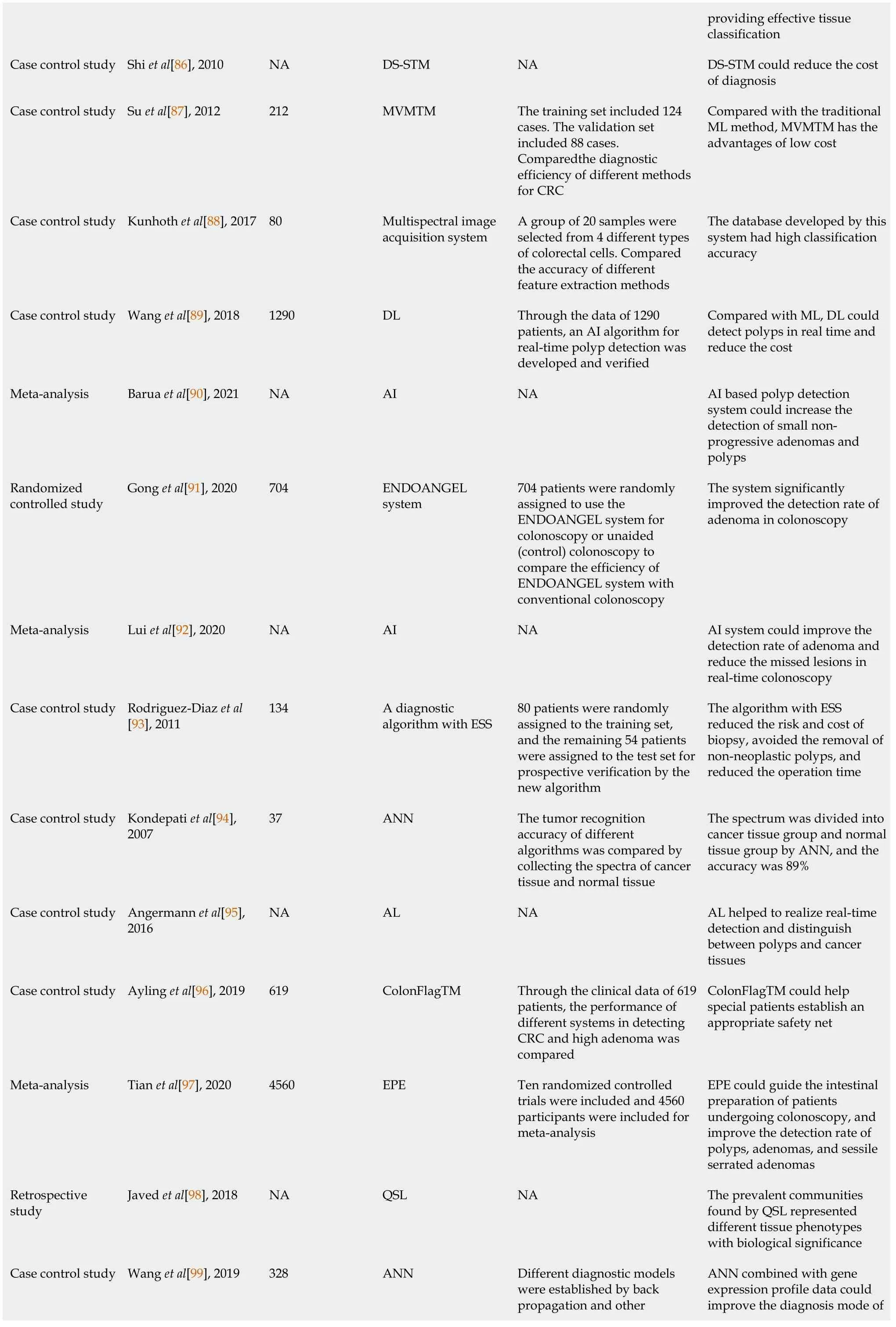
It is important to increase the sensitivity and specificity of early detection of CRC.First,massive endoscopic image datasets of early CRC should be set,with the early screening performed by colonoscopy and AI automatic recognition system.Second,early identification and timely warning for high-risk groups with a family history can be realized through new media and smartphone software.Third,with many pathological images and optical maps,we can identify whether the cutting edge is negative after endoscopic intervention in real time to adjust the treatment plan in time and avoid secondary surgery.Fourth,the government should establish a timely and effective national physical examination plan through AI to conduct early intervention and treatment for the high-risk population (Table 1).
After this, as many of the will-o -the-wisps as could get in crowded into Potentilla s garden, and by their light the tall yew-trees danced minuets until the Princess was weary and begged to be excused from looking at anything more that night
Although the consequence of CRC misdiagnosis is much more severe than that of polyp misdiagnosis,the research of CADe for CRC in CTC is still very limited[24].The reason may be that the lack of literature on the detection characteristics of early CRC[25] and the fact that it remains a problem to effectively distinguish masses from normal colonic anatomy based on the design features of mathematical images[24].Taylor
[25] collected the morphological characteristics of flat tumors by locating tumors to distinguish tumors from normal tissue structure and found that the CAD system combined with CTC was relatively effective for detecting flat (non-polypoid)cancer.CAD can improve the speed of image interpretation,find out the polyps missed by experts,reduce the variability between observers,and improve the sensitivity of polyp detection[26,27].However,the increase of FP generated by CAD may reduce the efficiency[22].Deep transfer learning can greatly improve the accuracy of polyp detection in CTC[28].Because the virtual intracavity images of polyp filtered by the CADe system can be used to modify the deep convolutional NN (DCNN)trained by millions of non-medical images,the DCNN can identify polyps[28].It can significantly improve the detection of polyps for inexperienced doctors using a visualization scheme in CTC.Combined with the CAD system,the visualization scheme can reduce radiologists’ interpretation time and improve the detection of colon tumors in CTC[29].Van Wijk
[30] presented a method by measuring the protrusion of candidate objects in a scale adaptive way to evaluate polyps larger than or equal to 6 mm,with a 95% sensitivity obtained.It was believed that identifying the size of polyps can reduce the risk of missed diagnosis of large polyps more than identifying the shape[30].Kim
[31] collected the CTC dataset interpreted by the CAD algorithm from polyp patients.The CTC dataset was designed to describe the lumpy structure extending into the lumen and could identify large polyps (>6 mm) with a high sensitivity and acceptable FP.Based on the characteristics of volume and shape,Nappi
[32] developed a CADe method to detect the location of colonic polyps and used this method to evaluate the serrated polyps confirmed by colonoscopy and biopsy.The results showed that the detection accuracy of the method was much higher than that of the traditional CADe system[32].Therefore,the application of CAD diagnosis has a promising prospect.However,more data sets and effective annotations are still needed to enhance the accuracy of AI diagnosis[21].
ML in imaging diagnosis
ML has to extract the most relevant or predictive features from many tested features and use these to determine the categories of new image samples[79,80].The features will help diagnose CRC in imaging.It is very important to segment colorectal tumors accurately in MRI images,while the manual or semi-manual method is very tedious,time-consuming,and operator-dependent[81].CAD plays an important role in many medical analyses,especially in computed tomography (CT) image analysis.Although many methods are designed,there are still some deficiencies in structure segmentation[82].Onder
[5] reported that ML methods including SVM and logistic regression could achieve better classification performance and improve the accuracy of the baseline CAD system.The ideal colon segmentation effect could be achieved in a CT image using the NN algorithm to remove the turbid liquid of the large intestine[83].Jian
[81] proposed a segmentation method based on the FCN framework.The normalization method was used to reduce the difference between images.The segmentation method could extract features from standardized images and generate corresponding predictions for reference using the idea of transfer learning.Finally,all predictions were fused to determine the final tumor boundary[81].Compared with manual segmentation of T2 weighted MRI images of CRC,the FCN based segmentation method had a higher accuracy.The FCN based segmentation method might replace the time-consuming manual method[81].In order to achieve accurate segmentation,a regression NN-augmented lagrangian genetic algorithm (RNNALGA) based on ML was proposed.Using RNN-ALGA,an accuracy of 97% could be achieved under the condition of small error.RNN-ALGA was suitable for abdominal CT image slices and could improve structural segmentation accuracy and time efficiency in diagnosing colonic diseases[82].
The troll, therefore, sentenced the king, either to answer three questions that he would put to him, or have his head taken off, as was agreed on in the old bond
ML in pathological diagnosis
Computational pathology based on AI and ML methods is most promising.The computer model has better image recognition ability than human experts[2].Largescale and high-quality training datasets are necessary for an ML-based image classifier to achieve high performance[84].ML-based tissue classification is a valuable method for manual histological analysis.However,high-resolution image classification is a complex and computationally expensive task.In addition,the goal of many tissue analysis tasks is to identify rare areas in the tissue.In colon cancer,tumor budding(TB) exists in the front of the tumor-infiltrating area,which is an important sign of tumor invasiveness[85].When the image is examined at a low resolution,the small objects are difficult or impossible to detect.Sun
[85] provided a two-tier CNN classification method that was explored to identify the small and important tissue areas in the whole slice tissue.The processing time of the method is reduced by 43%.The two-tier classifier provided an effective tissue classification by reducing the task area and increasing the chance of tumor bud recognition[85].A variety of serum tumor markers can be used in the diagnosis of CRC.There is a wide range of variability in the types and quantities of routinely used markers.The traditional single cut-off point also hinders the effective use of tumor markers.In order to improve the diagnosis accuracy and reduce the cost,it is important to optimize the inspection combination and make full use of the inspection value.Shi
[86] proposed an AI algorithm called diagnosis strategy of serum tumor maker,which proved that two markers were enough for diagnosis.Compared with SVM and decision tree,the multiple tumor markers with multiple cut-off values (MVMTM) algorithm could greatly improve the diagnosis efficiency of CRC using carcinoembryonic antigen,carbohydrate antigen 19-9 (CA19-9),and CA50[87].The establishment of an image database for colorectal tumor biopsy is an important step to detect the tumor.The automatic classification of tumor cells can improve the rapidity and accuracy of tumor diagnosis.Image processing and ML can be used to distinguish different cell types in digital biopsy sections.In addition to using conventional RGB/grayscale images,multispectral images often provide extensive information to support classification tasks.Kunhoth
[88] used a multispectral image acquisition system to develop a colorectal biopsy section database divided into training sets and test sets.In order to avoid the deviation,50 iterations were run,and the results of a single operation were averaged,which finally proved that the database had a high classification accuracy.The colorectal biopsy section database could help diagnose CRC[88].
A few days later, Timmy arrived back in school with a large bandage on his finger. With a big grin on his face, he walked up to me and said quietly, I m talking to my finger every day, wishing it well, and it s listening to me.
ML in endoscopic diagnosis
With good results in computer vision and other fields,ML still requires certain manual guidance[4].Removal of precancerous polyps is important for colon cancer prevention.However,the detection rate of adenomatous polyps is quite different among endoscopists[89].By calculating the risk and difference of detecting polyps,adenomas,and CRC,Barua
[90] compared colonoscopy with AI and colonoscopy without AI.It was found that an AI-based polyp detection system in colonoscopy could increase the detection rate of nonprogressive small adenomas and polyps but could not increase the detection rate of progressive adenomas[90].Wang
[89]developed the ENDOANGEL system and compared AI colonoscopy with colonoscopy without AI through random-control experiments.The results showed that AI significantly improved the detection rate of adenoma in colonoscopy[91].Lui
[92]suggested that the DL AI model could detect adenomas missed in routine colonoscopy in the real-time examination.They believed that the combination of AI and auxiliary equipment could eliminate the risk of missing lesions in colonoscopy when the intestine was well prepared[92].Elastic scattering spectroscopy (ESS) for optical guided biopsy had a high accuracy in tumor detection.Rodriguez-Diaz
[93]proposed two spectral classification frameworks,called ensemble classification and misclassification rejection,for clinical problems of non-tumor and tumor colorectal lesion classification based on ESS measurement.When the two frameworks were used to develop the diagnosis algorithm together,the classification effect would be better,and the medical cost would be reduced[93].Near-infrared spectroscopy could also be used to diagnose CRC and differentiate malignant tumors.Kondepati
[94]collected the spectrum of cancer tissue and normal tissue from colonic tissue with an optical fiber probe.Major spectral differences could be observed.The spectrum was divided into cancer tissue and normal tissue with an accuracy of 89% using ANN,linear discriminant analysis,and other pattern recognition methods[94].The method based on AL could perform real-time detection during colonoscopy and enhance detection performance at the same time.However,the possibility of increased FP made the algorithm difficult to use in daily clinical practice[95].Colon cancer might cause anemia as a common indication of colonoscopy.Hemoglobin concentration could be used as an indicator for the diagnosis of colon cancer,but it was not enough to diagnose colon cancer by hemoglobin concentration alone[96].The AI-based ColonFlagTM might be an appropriate indicator,which used all indicators of whole blood count,age,and gender.At the same time,ColonFlagTM could provide appropriate treatment suggestions for patients who did not accept the fecal examination or colonoscopy[96].Tian
[97] believed that enhanced patient education (EPE) can be realized through visual aids,telephone,mobile and social media applications,multimedia education,and other software.EPE was used to guide the intestinal preparation of patients with colonoscopy and improve the detection rate of polyps,adenomas,and sessile serrated adenomas[97].
The Fairy of the Beech-Woods ran to welcome the Prince and Princess with open arms, only too delighted to find them so much improved that she could, with a clear conscience, begin to spoil them again
QSL and SSL in diagnosis
The little tailor began his game once more, and flung the largest stone he could find in his wallet with all his force, and hit the first giant on the chest
The goal of the real-time endoscopic image diagnosis support system is to use AI during colonoscopy without interrupting the operation of any doctor[69].Based on the DL method,the real-time optical detection and analysis of polyps can be carried out by white light endoscopy alone[70].A real-time automatic polyp detection system can help endoscopists detect lesions that may correspond to adenomas quickly and reliably[13].The accuracy of endoscopic differential diagnosis enables the “resection and discard” mode of small-scale colorectal polyps[71].To relieve the high cost,long time consuming,and patients’ discomfort,Lund Henriksen
[71] explored a system for automatic polyp detection to assist and automate the examination procedures.By comparing root mean square propagation,stochastic gradient descent,and adaptive moment estimation,when stochastic gradient descent was used as the training optimizer,the detection rate increased while the number of FP was relatively stable[71].
USE OF AI IN TREATMENT OF CRC
AI in treatment decision
AI has become an irresistible trend in the medical field[108].At present,oncologists are familiar with clinical practice guidelines (CPGs) and provide follow-up treatment for patients based on CPGs.On the contrary,physicians may not be familiar with the guidelines[109].Passi
[109] developed a decision support system (DSS) that used CRC follow-up data as a source of knowledge to generate appropriate follow-up recommendations for patients.Passi
[109] designed and proposed the semantic framework of the web application,combining the current web technology and database storage with the designed ontology,and realized the unified development of DSS.Passi
[109] also designed a web application interface to provide doctors with the functions of CPGs.DSS development could help physicians and nurses provide postoperative care for CRC patients[109].Watson for Oncology provided oncologists with various cancer treatment suggestions,such as recommended,representing the preferred method;for consideration,not recommended.The absolute consistency of the treatment regimen with the recommendations of the multidisciplinary team of oncologists was studied.Lee
[110] used Watson for Oncology to process cases and compared the results with the actual treatment received by patients.Key findings included an increased consistency rate after multiple disciplinary team implementation,a low consistency rate in elderly patients,and a high consistency rate in patients receiving chemotherapy.The results proved that Watson for Oncology might be helpful to simulate the effect of multiple disciplinary teams.Using evidence-based guidelines and simplifying treatment pathways,multidisciplinary care could provide best practices[110].It is crucial to achieving personalized treatment since radiotherapy and chemotherapy are very painful.However,it is impossible to individualize patient treatment because the clinical situation of patients cannot easily link with DNA mutation[111].Siddiqi et al[111] designed a MATCH system that provided a unique combination of clinical and genetic sequence data and constructed a database for all users.The MATCH system was currently providing hundreds of data samples,including clinical information,tumor markers,proteome sequences,gene inhibitors,etc.The importance of all data attributes and the corresponding processing information were modifiable[111].Moreover,the system was developed with web services,which guaranteed interoperability among hospitals,pharmaceutical laboratories,and research centers,allowing them to access and exchange samples,information,and data models.The MATCH system helped identify the correlation between medical features so that oncologists could understand each patient’s individual situation[111].Nanorobots are expected to become intelligent drug delivery systems that respond to small molecular triggers[112].Felfoul et al[113] developed a nanorobot that could deliver drugs to cancer cells.The robot sensed the concentration of hypoxia and delivered drugs in the “anoxic area” generated by the active proliferation of cancer cells.The robot achieved an accurate effect of attacking cancer tumors[113].Li et al[112] developed a nanorobot,which could kill cancer cells by releasing procoagulant substances in the cancer tissue,interrupting the blood supply to the cancer tissue.The greatest progress of robots is that it can significantly improve the targeting of chemotherapy drugs and reduce the killing effect of chemotherapy drugs on human normal tissues.
ML in immunotherapy pathway
Computational pathology can help obtain complete and repeatable datasets to promote individualized prediction of immunotherapy.ML can help evaluate the expression of immunohistochemical markers,tumor morphology,and the spatial distribution of tumor-infiltrating lymphocytes.The methylome group features queried by ML are proved to be suitable for predicting the response to immunosuppressive checkpoint inhibitors.Similar to image analysis,this method considers both tumor cells and reactive cells.The immune profiling is detected by spatial analysis and multiplexing of tumor immune cell interaction,and it is used as a predictor of patients’response to cancer treatment[114].ML can be used to inhibit the Wnt/beta-catenin signaling,which is beneficial in cancer therapy[115],and it has the potential to provide new therapeutic strategies for patients by recognizing the interaction of tumor cells[114].
AI in endoscopic and surgical therapy
The estimation of the invasion depth is an important step in successfully implementing endoscopic submucosal dissection[116].At present,narrow-band imaging with magnifying endoscopy is a practical method to estimate the invasion depth of CRC.Lee
[116] used AI to interpret the cell endoscope images.Processing thousands of images,the algorithm could diagnose more than 90% of invasive CRC in hundreds of images detected[116].Although the incidence of lymph node metastasis is relatively low,most T1 CRCs still need to undergo colectomy and lymphadenectomy[117].Ichimasa
[117] used the data of hundreds of patients in the AI model.The model analyzed 45 clinical and pathological factors and predicted positive or negative lymph node metastasis.The operation specimen is the gold standard of lymph node metastasis.Model validation results showed that patients received many unnecessary surgeries without lymph node metastasis[117].AI can reduce unnecessary surgeries after endoscopic resection of T1 CRCs by predicting the presence of lymph node metastasis[117].
15.Ball:A ball is a large party in which the participants dress up in their finest clothes and dance. Balls were exclusively for the privileged and wealthy.
Compared with open surgery,a minimally invasive one is superior in short-term prognosis and long-term efficacy[118].With the increasing popularity of laparoscopic surgery,the number of robotic surgeries is also growing.Surgeons can control the robot system 100% and perform more accurate operations at any time[119].Kim[119]reported an animal experiment in which the effect of using smart tissue autonomous robots was comparable or even superior to open surgery,laparoscopic surgery,or robotic surgery[119].The smart tissue autonomous robot integrates the sewing tool,robot arm,force sensor,and camera in hardware and software.The robot has the ability to stitch soft tissue.The efficiency of the robot sutured on the plane was 5 times faster than that of the surgeons,and 9 times faster than that of the surgeons using laparoscopic manual tools.Experiments also showed that the stitching robot was more accurate and consistent[120].Compared with the Da Vinci Si robot system,the new Da Vinci Xi increased more flexibility of operation,and it was expected to promote the performance of multi quadrant surgery[121].The clinicopathological characteristics and perioperative outcomes of patients with two kinds of robot systems were analyzed.The results showed that the ileostomy rate of Xi group was low,the operation time was short,the amount of bleeding was small,and the recovery was fast[121].Surgeons can input operation instructions,order medical robots to perform complicated operations,and constantly monitor the operation on the monitor.During the operation,the surgeon can see the anatomical structure without opening the abdomen.Because the fluorescent dye is injected before the operation,the malignant cells and tissues can be visible.As a result,doctors can remove lesions more precisely[119].Because of the precise recognition and detailed operation of robotic surgery,the learning curve of robotic colorectal surgery is shorter than that of laparoscopic surgery.
Robotic surgeries are beneficial in minimally invasive surgery of tumors,such as high-resolution and stable 3D views,optimal
free movement,and elimination of natural tremors[118].However,in the face of a real surgical suture,the robot exposes its limitations.The complex structure of the human body requires the robot to spend much time processing information about the anastomosis,which is obviously not beneficial in the time-consuming operation.Therefore,improving the image recognition and processing ability of the robot is the right direction to improve and develop the robot’s autonomous stitching[120].Compared with traditional laparoscopic surgery,robot surgery has some benefits,such as less urinary and sexual dysfunction and less intraoperative blood loss
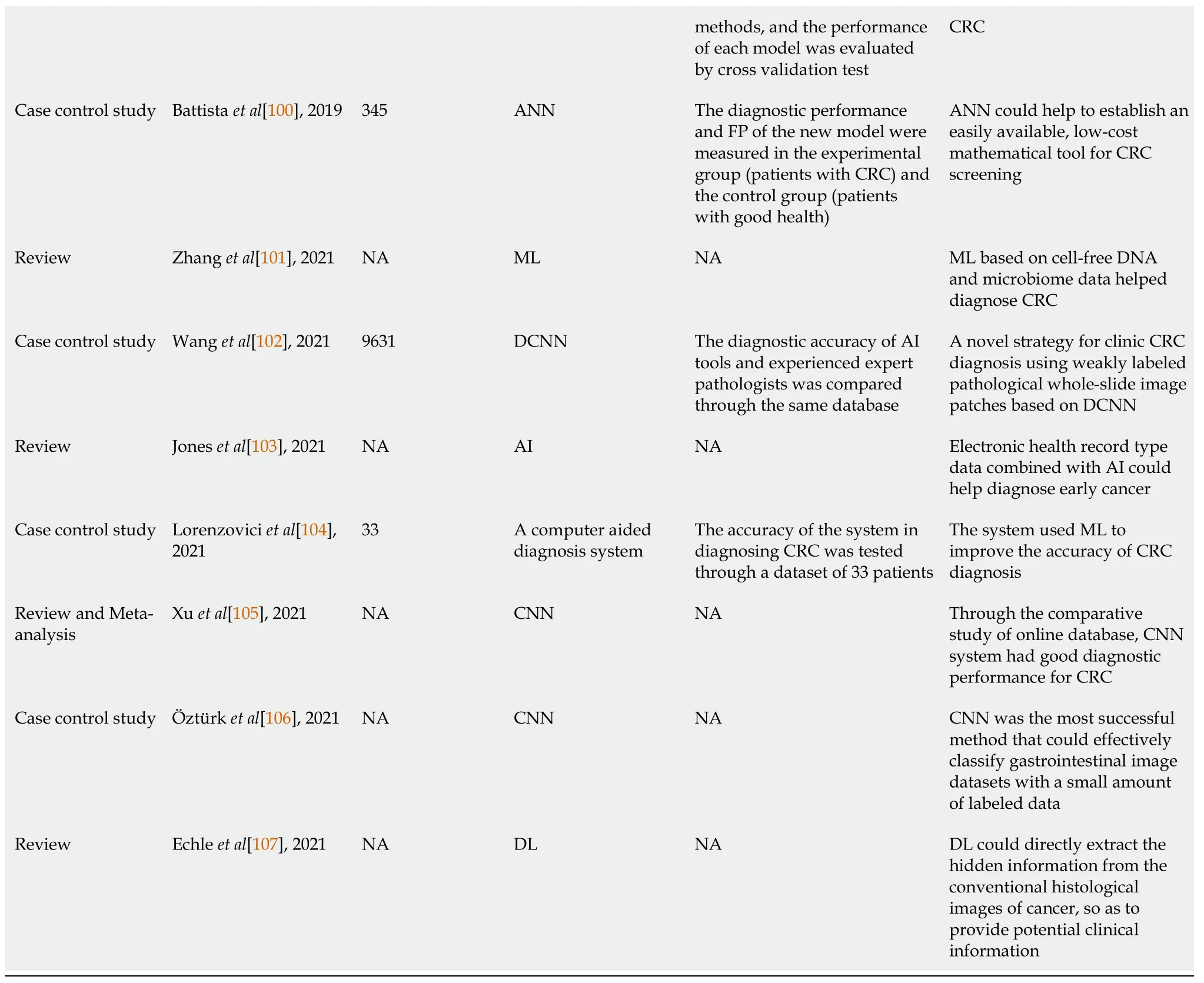
However,more powerful evidence is needed[122].Due to the high cost of robot,it will take a while to collect the data of robot surgery.However,as competition can decrease the price of robotic surgical systems,its promotion will be accelerated in the future.In robotic CRC surgery,many limitations have presented,such as the lack of unified technical standards and excessive dependence on surgical robot equipment.The problems will be solved by establishing training system and integrating medicine,research,and production.During clinical studies and large data analysis,robotic surgery will be the new development trend of colorectal surgery[122].Other studies also described the application of AI in the therapy of CRC[123-127] (Table 2).
USE OF AI IN PROGNOSIS EVALUATION OF CRC
If CRC is detected early,it is almost curable.However,in order to make a correct diagnosis,a double examination of biopsy and colonoscopy image is required,so the cost of diagnosis has increased[39].Thus,the use of DL and automatic image analysis in pathology is increasing,which is called the third revolution of pathology[40].Although the automatic coding in DL is considered helpful in extracting multi-layer image features and deep NNs can classify the features,it takes much time to train artificial neurons[41].
ML in prognosis evaluation
The molecular subtype of CRC can be used as a prognostic indicator of relapse-free survival rate.The determination of molecular subtype depends on the analysis of hundreds of genes[136].Popovici
[136] proposed a method to recognize CRC molecular subtypes from conventional histological images based on an SVM classifier.They used the DCNN to extract the local descriptors and then construct the dictionary representation of each tumor sample.A set of SVM classifiers were trained to solve different binary decision problems.The combined output was used to predict the molecular subtype.The overall accuracy of the results was very high[136].It was beneficial to improve the accuracy of prognosis prediction.Zhang e
[128] collected genetic variation and environmental information of CRC patients and cancer-free controls,trained the model with the large data,and established a multi-method integrated model.The model could effectively predict CRC risk[128].The improved heterogeneous integrated learning model and generalized kernel recursive maximum correlation entropy algorithm had higher prediction ability than SVM[128].ML is used to extract disease prediction models from electronic medical records[137].ML can also solve many electronic medical record data,such as timeliness,imprecision,and integrity[129,138].Hoogendoorn
[137] could extract useful information from consulting notes,and the prediction performance of the ontology-based extraction method was significantly beyond the age and gender benchmark.It has been proved that the best way to predict CRC is by linking medical record texts with medical concepts[137].
The visual estimation of stroma ratio in microscopic images provides a strong predictor of survival rate in patients with CRC[139,140].However,visual assessment is highly influenced by the observer and interstitial variation.Based on supervised learning,an objective quantitative method of tumor and stroma was established.Compared with the visual estimation of pathologists,the automatic tissue quantitative method was reliable and practical because it provided a new way to evaluate the prognosis and was crucial to predicting the tumor’s survival ability[139].Wang
[141] developed a two-stage model to predict the survival of patients with advanced cancer.The first stage predicted whether patients could survive for more than 5 years.The second stage predicted the exact survival time of patients who could not survive for 5 years (in months).With low prediction error and good generalization performance,the two-stage model could help make treatment decisions,improve patient satisfaction,save medical resources,and reduce medical costs[141].Based on the knowledge representation method of probability,Oliveira
[142] designed a Clinical Decision Support System (CDSS) which,based on the cancer patients’ records and the precise knowledge of experts,could propose an effective treatment scheme and solve the uncertainty of prognosis after surgery[142].CDSS could complete four basic tasks:Data organization,data collection,the combination of various principles and specific data,and user-friendly display of analysis results.CDSS screened out appropriate treatment methods from the aspects of curative effect,total survival rate,and side effect rate[143].By comparing the treatment and prognosis of 250 cancer patients,Aikemu
[124] found that Watson for Oncology could replace oncologists to provide patients with cutting-edge medical research and knowledge to a certain extent.It was also believed that the use of Watson for Oncology and other decision support tools could help achieve the promise of precision medicine[124].
Although resection of colon polyps can reduce the incidence rate and mortality of CRC by 75%,there is no individualized surveillance plan for polyp recurrence risk.Harrington
[144] extracted polyp features from colonoscopy and pathological reports.The features extracted from these records and other demographic and anthropometric information were used to develop and compare ML models to predict polyp recurrence.The evaluation of the ML model further emphasized the important characteristics of predicting polyp recurrence from population and health records.RF model could detect patients with a high risk of recurrence and promote frequent follow-ups[144].It is of great significance for individualized medical treatment.In order to improve the classification of polyps,Xie
[145] proposed biometric modeling and ML methods to build polyp classifiers and screened the results of colonoscopy in a Chinese formation.The results showed that the RF model could improve the prediction performance compared with other methods[145].Xie
[145] also provided evidence that emotional state might be an influential factor in the early growth of CRC in China.
DL in prognosis evaluation
A deep network can directly predict the prognosis of CRC according to the morphological characteristics of tumor tissue samples[61].Patients with CRC will benefit from the detection of TB,which is a reliable prognostic biomarker.DL can greatly reduce the number of FPs by detecting TB in H&E stained sections[146].Zhao
[147]proposed a DL model for automatic tumor-stroma ratio quantification using HE staining images of CRC.The model could eliminate the errors caused by traditional visual evaluation and reduce the work intensity of pathologists.Therefore,Zhao
[147] believed that the model was suitable for clinical practice and might be helpful for clinical prognosis prediction and decision-making.Multimodal Deep Boltzmann Machine (DBM) is a DL structure used to predict patients' survival time.Syafiandini
[148] integrated gene expression and clinical data into a new data form.The new data had few eigenvalues.In the multi-mode DBM architecture,these data were extracted from the joint hidden layer to identify gene subtypes,predict the response to a certain treatment,and find the most suitable treatment for patients[148].Roadknight
[149] described a dataset on the cellular and physical conditions of CRC patients who underwent surgical resection.These data provided unique immune status information for tumor resection,tumor classification,and postoperative survival[149].Roadknight
[149] studied the clustering and ML of these data to prove that the integrated method could predict the prognosis of patients.Compared with SVM,the better way to predict the tumor-node-metastasis stage from immunohistochemical markers is to use the anti-learning method[149].Compared with other algorithms,the anti-learning method can more accurately predict cancer stage and survival rate from immune attributes[6].
Although optical biopsy is a promising field,tissue biopsy remains the gold standard.Whether the surface microstructure accurately reflects the histological characteristics of lesions will affect the results of optical biopsy[3,13,72,73].The widespread clinical use of microscopic technology,especially the combination of virtual chromoendoscopy and microscopic imaging,has brought more attention to the field of optical biopsy[74].Endoscopists can reliably diagnose and differentiate microadenomatous and hyperplastic polyps using established optical evaluation criteria[75].The development of CAD and AI algorithms may overcome the main obstacles of optical biopsy and change the treatment of colorectal lesions[74,76].Endocytoscopy is an effective method for deep diagnosis of CRC because of the high resolution[73].Kudo
[77] developed an AI-based system called EndoBRAIN which could identify the colon tumor by analyzing the nucleus,crypt structure,and microvasculature in the endoscopic image.The initial training of EndoBRAIN was carried out using endoscopic images.The diagnostic efficiency of endoscopists and the diagnostic performance of EndoBRAIN were analyzed retrospectively.The result showed that EndoBRAIN could increase the accuracy of the diagnosis[77].Mahmood
[78]proposed a new monocular endoscope depth estimation and terrain reconstruction system,which took advantage of the joint training framework based on CNN and conditional random field.The system used the synthetic endoscope data for training and the colon model data for fine-tuning.It could be integrated into the endoscope system,which provided a basis for improving the CAD algorithm to detect,segment,and classify lesions[78].
SSL in prognosis evaluation
SSL methods use labeled or unlabeled data and graph regularization to predict patient survival and cancer recurrence[150,151].The data of gene expression is transformed into the graph structure of SSL,and the data of protein interaction and gene expression are integrated to select gene pairs[151].SSL methods can result in more accurate prediction than traditional SVM[11,150].Recognition of cancer-related mutations is essential for understanding the cancer genomes that cause cancer gene activation or tumor suppressor gene inactivation[152].Du
[152] proposed a new feature selection method based on supervised learning that could identify gene mutations.The model was composed of the best features in candidate features’ set with rotation forest.The method had a high accuracy and high prediction performance[152].Chi
[153] used the semi-supervised logistic regression method to establish the clinical prediction model of CRC survival risk.The performance of the model was strictly compared with that of other supervised learning models[153].The model of CRC survival risk prediction established by the SSL method had good correction ability,popularization,interpretability,and clinical practicability.Other commonly used supervised learning methods,such as SVM,RF,and NN,showed poor calibration performance[153].The SSL model might have more potential to develop a better risk prediction model in the actual clinical environment than the supervision model[153].
QSL eliminates the need for traditional supervised learning for manual labeling and reduces expert intervention.QSL texture labeling may be useful in the analysis and classification of pathological sections,but further research is needed[5].The main purpose of analyzing millions of pixel histological images is to help pathologists predict cancer.At present,most methods are limited to the classification of tumors and stroma.Moreover,most of the existing methods are based on fully supervised learning and require many annotations that are difficult to obtain[98].Javed
[98] proposed a new group detection algorithm based on SSL,which could identify six different phenotypes in millions of pixels of image data.Two independent CRC datasets showed that the SSL algorithm was superior to the latest method[98].ANNs are a class of models inspired by biological NNs,which are used to estimate functions that depend on a large number of general unknown inputs[99].ANNs are usually shown as interconnected neuron systems,exchanging information with each other.Each connection has a digital weight,adjusted according to experience to make the input flexible and learn[4,9,99].The establishment of diagnosis models based on ANN is helpful for clinicians to diagnose CRC,predicting postoperative outcomes,and screening high-risk prognosis subgroups[99].ANNs have a good prospect in the general survey of CRC by establishing a clinical data model.This method is simple,low-cost,and non-invasive[100].Other studies also described the application of AI in the diagnosis of CRC[101-107].
Other algorithms of AI in prognosis evaluation
The CRC recurrence support (CARES) system guided the prognosis by comparing the patients with new CRC and those with previous CRC to determine the high-risk group.As a result,only high-risk patients could receive more stringent examinations with reduced medical costs,while low-risk patients could be free from frequent and unnecessary examinations[154].Immune cores could predict the prognosis of patients with colon cancer,and AI could detect additional prognostic markers on pathological sections.Digital tumor parameters (DGMate) were used to detect the digital parameters related to prognosis in tumor cells.The higher density of CD3+ tumor core,CD3+ invasive margin,and CD8+ tumor core was found,and the longer relapsefree survival was reported.CD3+ tumor core had a similar value to the classical CD3/CD8 immune core in prognosis.It was indicated that AI could help pathologists determine the prognosis of patients with colon cancer,which might improve patient treatments[155].The existing methods describe the coordination among multiple genes by the additive representation of expression spectrum and use a fast heuristic method to identify the disjointed subnetworks.The methods may not be suitable for the potential combination of the disjointed genes[156].Chowdhury
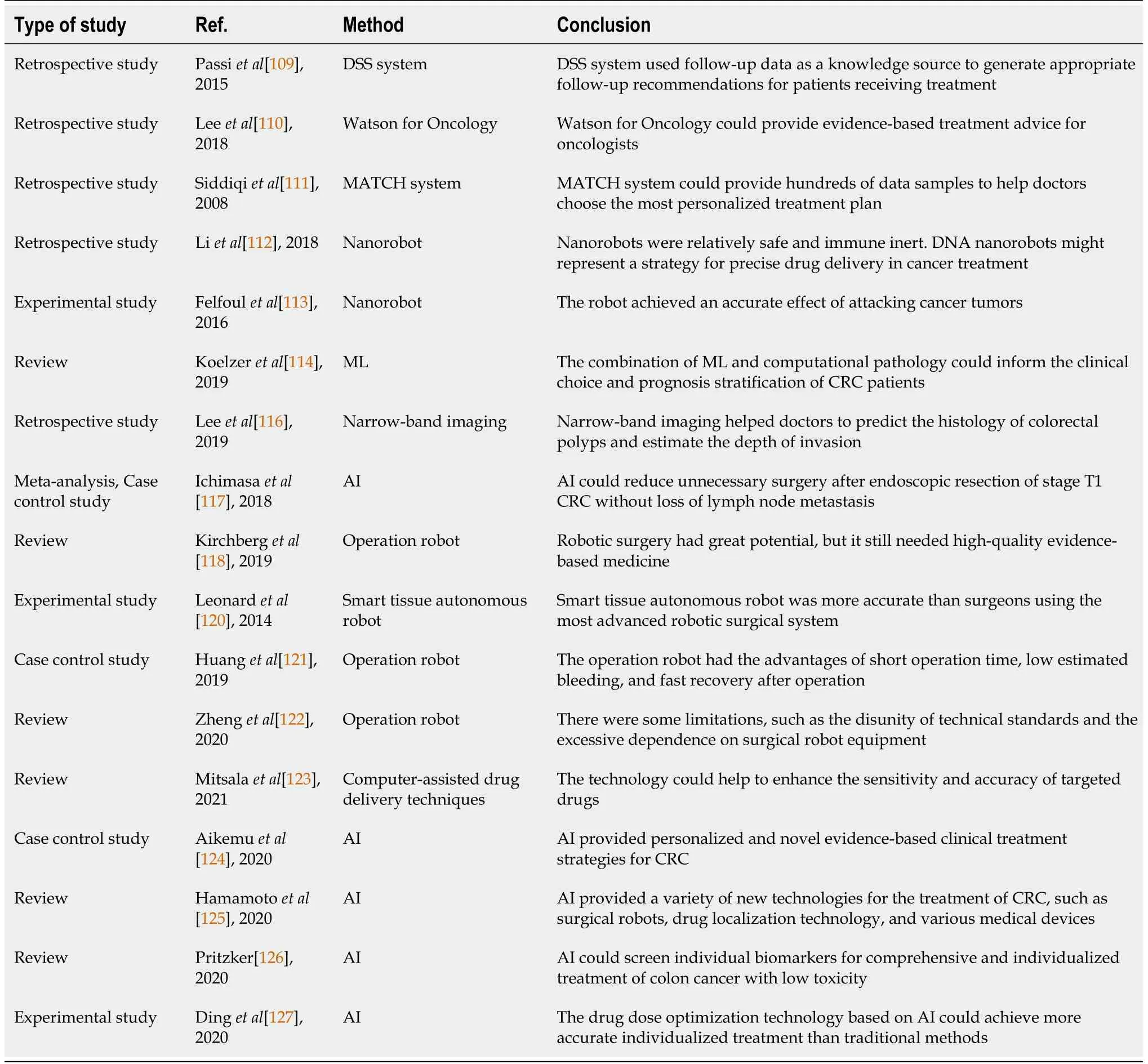
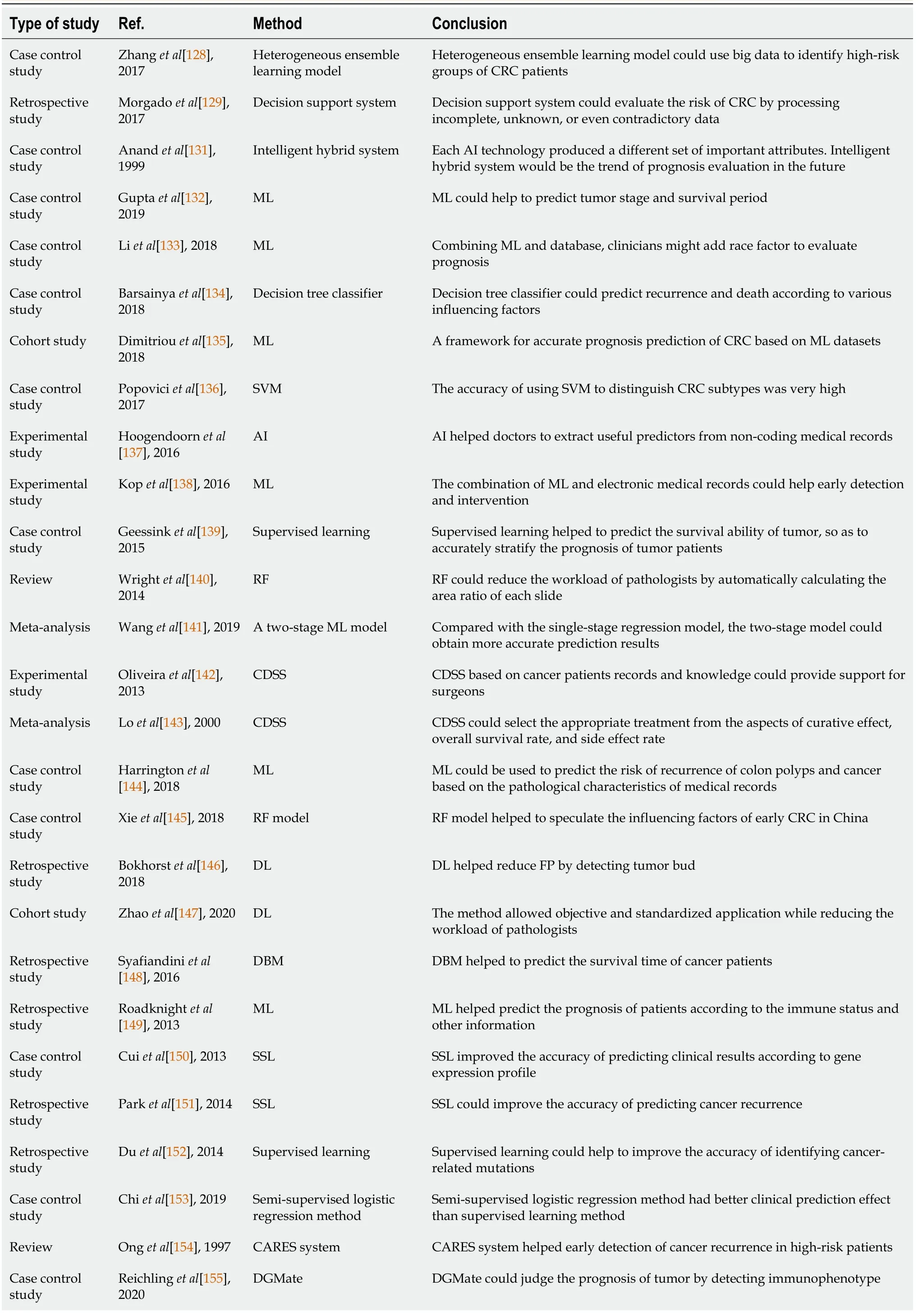
[156] designed the Crane algorithm to solve this problem and proposed that the Crane algorithm was better than the addition algorithm in predicting CRC metastasis.In addition,AI could also be used to build CRC education software,whose menu contained an introduction,signs and symptoms,risk factors,preventive measures,and CRC screening procedures.The education software could achieve publicity and popularization of common sense through the communication between clinicians and patient representatives[157].Other study also described the application of AI in the prognosis of CRC[158] (Table 3).

DISCUSSION
AI plays an important role in the fields of computer,internet,and vehicle engineering.The four main directions of future medical development are “personalization,precision,minimal invasion,and remoteness”[159].In the field of medicine,first,AI gradually shows its advantages in disease diagnosis,treatment,and prognosis.CRC is one of the common human cancers,and its early diagnosis and standardized treatment have a profound impact on the prognosis.The development of AI for CRC has gone through the following stages:(1) Understanding cancer at the molecular and cellular levels through DL;(2) Assisting in the diagnosis of CRC according to images and pathological specimens;(3) Clinical drug designing and screening;and (4) Promoting the individualization of CRC diagnosis and treatment[159].The diagnosis of CRC is mainly divided into imaging diagnosis and pathological diagnosis.Most of the imaging datasets are objective datasets with a high degree of information standardization.The CAD system based on DL realizes the automatic analysis and optimization of diversified images by extracting features from experts,extensive image training,making classification rules,and establishing mathematical models.Second,AI is beneficial to medical image analysis.Highly efficient image processing and analysis speed can quickly give auxiliary judgment results.Good sensitivity can reduce the missed diagnosis rate.Expert knowledge learning and quantitative data analysis can improve the quality of the basic inspection.Third,in clinical pathology,many digital sections of CRC have been accumulated,and some have been preliminarily developed with the technology of image recognition and DL.However,at present,AI cannot be separated from the auxiliary role.AI application at the functional level mainly includes disease diagnosis support and treatment decision support.The development of disease diagnosis support is active in treatment decision support.Advanced technologies are integrated with medicine and gradually play a necessary role in assisting diagnosis and early screening of major diseases.
Although AI is developing rapidly,it is still in the experimental stage and still faces many development bottlenecks.For example,first of all,the development of AI overemphasizes “probability association,” but diseases always exist in unknown areas.How to combine data and medical knowledge is the key to the development of image AI.Second,AI-based DL requires much label data for training.Although labeled data has more influence on training results than algorithms,high-quality data acquisition for training is a big problem.Third,the image data standardization is low.The level of image system interaction operation in different hospitals is low.Moreover,the datasets of each imaging system are scattered all over the country with a low level of interaction.Forth,the difficulty of data annotation is great.The AI training requires a large amount of labeled image data,and the annotation needs to spend a lot of manual costs,which directly impacts the training results.
Meanwhile,the “black box” problem in ML raises several concerns clinically.ML can help read imaging and pathological pictures,recommend diagnosis and treatment options,and predict prognosis.However,due to the “black box” problem,the clinical application of AI tools progressed slowly.To further develop AI medicine,it is necessary to improve the interpretability of ML algorithms.The small steps of biological interpretation and clinical experience in ML algorithm can gradually solve the “black box” problem.In order to solve the above problems,data preprocessing is needed to complete the standardization,which requires the integration and fusion of heterogeneous data sets,such as images,physiological data,and information texts.At the same time,automatic software is used to analyze the medical image data quantitatively and extract a large number of features,including texture analysis,shape description,and other quantitative indicators.
The treatments for CRC are mainly surgery and chemotherapy.AI enables individual precision medicine by selecting appropriate treatment measures through big data analysis and comparison.At the same time,the development of robot technology provides a guarantee for the high accuracy of surgery and the high targeting of chemotherapy drugs.However,the quality of the data collection is still not enough to support AI to make treatment decisions independently.The complexity of the human body also reduces the speed of analysis and decision-making of AI in operations.In addition,robots cannot be widely used because of the high economic cost.Patients are often afraid of the unknown survival period after surgery,so giving a specific survival period can eliminate the psychological burden of patients.AI can predict the survival time and recurrence risk through patient information,surgery,and pathology and guide patients’ prognosis and nursing.Therefore,high-quality,accurate data and standard operating specifications are required.In other words,the accuracy of prediction risk depends on the quality of the prognosis data,which in turn depends on the quality of data generated by diagnosis and treatment.
Additional authors on the American Mineralogist paper, Panguite, (Ti4+,Sc,Al,Mg,Zr,Ca)1.8O3, a new ultra-refractory titania mineral from the Allende meteorite: Synchrotron micro-diffraction and EBSD, are John R. Beckett, senior research scientist at Caltech; Oliver Tschauner from the University of Nevada-Las Vegas; and Wenjun Liu from the Argonne National Laboratory. The study was supported through grants from the National Science Foundation, the U.S. Department of Energy, and NASA s Office of Space Science.
When he got up he salaamed to it, who returned his greeting with joy and gratitude145, and caressed him and said: O youth, tell me true! who are you, and where are you going? And how did you cross that pitiless desert where never yet foot of man had trod? The prince told his story from beginning to end, and finished by saying: Now it is my heart s wish that you should help me to get to Waq of the Caucasus
As diagnostic technology evolves,the information available to doctors is becoming more and more complex.In terms of treatment,new drugs are constantly developed,and new treatment schemes and methods are emerging.It is challenging for busy clinicians to have enough time and energy to obtain,screen,and use the information.With the continuous development of AI technology and image recognition,and the continued improvement of other aspects,AI will play an important role in CRC diagnosis and treatment.Therefore,the establishment of an AI standard system will be the top priority of future development.The standardization of images,features,medical record information,and other datasets will improve the accuracy of diagnosis and treatment.DL and ML will fully be combined to enable robots to complete surgery independently.Medical services include not only medical technology but also the guidance of patients’ mental health.In the future,robots will provide nursing and adjust the psychological state of patients.However,moral and ethical issues must be well considered for the proper use of AI robots in today’s medical environment.
Various countries have been trying to establish ethical,legal,and regulatory compliance standards for AI development.But there are many difficulties before fully accepting AI robots.First,patients’ trust and acceptance will become an important factor in developing AI robotic surgery.The “black box” that has been used in many non-surgical applications has little theoretical transparency.In the medical field,lack of transparency impairs the doctors and patients' trust and acceptance of AI.Second,the safety of AI robot surgery is still an important issue to be concerned.The development of AI robot surgery involves a series of security problems,such as patient information protection,network security,robot autonomy,and machine failure.If the control of the AI robot is lost due to external factors such as network transmission delay and hacker attack,the immeasurable loss will happen.Third,the responsibility attribution of medical malpractice remains a problem.Given the limitations of AI robots,the issues of medical malpractice responsibility will lead to a debate about the gray area of law.The solution of this problem will boost AI development[160].
CONCLUSION
Currently,AI is in the era of weak AI and does not have communication capabilities.Therefore,the current AI technology is mainly used for image recognition and auxiliary analysis without in-depth communication with patients.With the continuous development of AI technology,the role of AI in the diagnosis and treatment of CRC will continue to increase until the robot can complete surgery independently.At that time,AI will change the medical technologies and even the medical model.
We thank the anonymous referees for their useful suggestions.
1 Sivapalaratnam S.Artificial intelligence and machine learning in haematology.
2019;185:207-208 [PMID:30729496 DOI:10.1111/bjh.15774]
2 Acs B,Rantalainen M,Hartman J.Artificial intelligence as the next step towards precision pathology.
2020;288:62-81 [PMID:32128929 DOI:10.1111/joim.13030]
3 El Hajjar A,Rey JF.Artificial intelligence in gastrointestinal endoscopy:general overview.
2020;133:326-334 [PMID:31929362 DOI:10.1097/CM9.0000000000000623]
4 Min JK,Kwak MS,Cha JM.Overview of Deep Learning in Gastrointestinal Endoscopy.
2019;13:388-393 [PMID:30630221 DOI:10.5009/gnl18384]
5 Onder D,Sarioglu S,Karacali B.Automated labelling of cancer textures in colorectal histopathology slides using quasi-supervised learning.
2013;47:33-42 [PMID:23415158 DOI:10.1016/j.micron.2013.01.003]
6 Roadknight C,Aickelin U,Qiu G,Scholefield J,Durrant L.Supervised learning and anti-learning of colorectal cancer classes and survival rates from cellular biology parameters.Proceedings 2012 IEEE international conference on systems,man,and cybernetics.2012:797-802 [DOI:10.1109/icsmc.2012.6377825]
7 Chen Y,Carroll RJ,Hinz ER,Shah A,Eyler AE,Denny JC,Xu H.Applying active learning to high-throughput phenotyping algorithms for electronic health records data.
2013;20:e253-e259 [PMID:23851443 DOI:10.1136/amiajnl-2013-001945]
8 Le Berre C,Sandborn WJ,Aridhi S,Devignes MD,Fournier L,Sma?l-Tabbone M,Danese S,Peyrin-Biroulet L.Application of Artificial Intelligence to Gastroenterology and Hepatology.
2020;158:76-94.e2 [PMID:31593701 DOI:10.1053/j.gastro.2019.08.058]
9 Jagga Z,Gupta D.Machine learning for biomarker identification in cancer research-developments toward its clinical application.
2015;12:371-387 [PMID:29771660 DOI:10.2217/pme.15.5]
10 Low SK,Nakamura Y.The road map of cancer precision medicine with the innovation of advanced cancer detection technology and personalized immunotherapy.
2019;49:596-603[PMID:31135897 DOI:10.1093/jjco/hyz073]
11 Shi M,Zhang B.Semi-supervised learning improves gene expression-based prediction of cancer recurrence.
2011;27:3017-3023 [PMID:21893520 DOI:10.1093/bioinformatics/btr502]
12 Gulati S,Patel M,Emmanuel A,Haji A,Hayee B,Neumann H.The future of endoscopy:Advances in endoscopic image innovations.
2020;32:512-522 [PMID:31286574 DOI:10.1111/den.13481]
13 Wang P,Berzin TM,Glissen Brown JR,Bharadwaj S,Becq A,Xiao X,Liu P,Li L,Song Y,Zhang D,Li Y,Xu G,Tu M,Liu X.Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates:a prospective randomised controlled study.
2019;68:1813-1819[PMID:30814121 DOI:10.1136/gutjnl-2018-317500]
14 Kang J,Gwak J.Ensemble of instance segmentation models for polyp segmentation in colonoscopy images.
2019;7:26440-26447 [DOI:10.1109/access.2019.2900672]
15 Eisner R,Greiner R,Tso V,Wang H,Fedorak RN.A machine-learned predictor of colonic polyps based on urinary metabolomics.
2013;2013:303982 [PMID:24307992 DOI:10.1155/2013/303982]
16 K?küer M,Naguib RN,Jancovic P,Younghusband HB,Green RC.Cancer risk analysis in families with hereditary nonpolyposis colorectal cancer.
2006;10:581-587[PMID:16871728 DOI:10.1109/titb.2006.872054]
17 Bell CS,Puerto GA,Mariottini G-L,Valdastri P.Six DOF motion estimation for teleoperated flexible endoscopes using optical flow:A comparative study.2014 IEEE international conference on robotics and automation.2014:5386-5392 [DOI:10.1109/icra.2014.6907651]
18 Liu Z,Wang S,Dong D,Wei J,Fang C,Zhou X,Sun K,Li L,Li B,Wang M,Tian J.The Applications of Radiomics in Precision Diagnosis and Treatment of Oncology:Opportunities and Challenges.
2019;9:1303-1322 [PMID:30867832 DOI:10.7150/thno.30309]
19 Yang T,Liang N,Li J,Yang Y,Li Y,Huang Q,Li R,He X,Zhang H.Intelligent imaging technology in diagnosis of colorectal cancer using deep learning.
2019;7:178839-178847 [DOI:10.1109/access.2019.2958124]
20 Dalca A,Danagoulian G,Kikinis R,Schmidt E,Golland P.Sparse classification for computer aided diagnosis using learned dictionaries.Medical Image Computing and Computer-Assisted Intervention,2011:537-545
21 Regge D,Halligan S.CAD:how it works,how to use it,performance.
2013;82:1171-1176 [PMID:22595503 DOI:10.1016/j.ejrad.2012.04.022]
22 Summers RM,Handwerker LR,Pickhardt PJ,Van Uitert RL,Deshpande KK,Yeshwant S,Yao J,Franaszek M.Performance of a previously validated CT colonography computer-aided detection system in a new patient population.
2008;191:168-174 [PMID:18562741 DOI:10.2214/AJR.07.3354]
23 Chowdhury TA,Whelan PF,Ghita O.A fully automatic CAD-CTC system based on curvature analysis for standard and low-dose CT data.
2008;55:888-901 [PMID:18334380 DOI:10.1109/TBME.2007.909506]
24 Nappi JJ,Hironaka T,Yoshida H.Detection of colorectal masses in CT colonography:Application of deep residual networks for differentiating masses from normal colon anatomy.Medical imaging 2018:Computer-aided diagnosis.Bellingham:Spie-Int Soc Optical Engineering,2018 [DOI:10.1117/12.2293848]
25 Taylor SA,Iinuma G,Saito Y,Zhang J,Halligan S.CT colonography:computer-aided detection of morphologically flat T1 colonic carcinoma.
2008;18:1666-1673 [PMID:18389248 DOI:10.1007/s00330-008-0936-7]
26 Summers RM.Current concepts in computer-aided detection for CT colonography.2010 7th IEEE international symposium on biomedical imaging:From nano to macro.2010:269-272 [DOI:10.1109/isbi.2010.5490363]
27 Lee JG,Hyo Kim J,Hyung Kim S,Sun Park H,Ihn Choi B.A straightforward approach to computer-aided polyp detection using a polyp-specific volumetric feature in CT colonography.
2011;41:790-801 [PMID:21762887 DOI:10.1016/j.compbiomed.2011.06.015]
28 Nappi JJ,Hironaka T,Regge D,Yoshida H.Deep transfer learning of virtual endoluminal views for the detection of polyps in CT colonography.Medical imaging 2016:Computer-aided diagnosis.Bellingham:Spie-Int Soc Optical Engineering,2015 [DOI:10.1117/12.2217260]
29 N?ppi J,Frimmel H,Yoshida H.Virtual endoscopic visualization of the colon by shape-scale signatures.
2005;9:120-131 [PMID:15787014 DOI:10.1109/titb.2004.837834]
30 van Wijk C,van Ravesteijn VF,Vos FM,van Vliet LJ.Detection and segmentation of colonic polyps on implicit isosurfaces by second principal curvature flow.
2010;29:688-698 [PMID:20199908 DOI:10.1109/TMI.2009.2031323]
31 Kim SH,Lee JM,Lee JG,Kim JH,Lefere PA,Han JK,Choi BI.Computer-aided detection of colonic polyps at CT colonography using a Hessian matrix-based algorithm:preliminary study.
2007;189:41-51 [PMID:17579150 DOI:10.2214/AJR.07.2072]
32 Nappi JJ,Pickhardt P,Kim DH,Hironaka T,Yoshida H.Deep learning of contrast-coated serrated polyps for computer-aided detection in CT colonography.Medical imaging 2017:Computer-aided diagnosis,2017 [DOI:10.1117/12.2255634]
33 Ma J,Dercle L,Lichtenstein P,Wang D,Chen A,Zhu J,Piessevaux H,Zhao J,Schwartz LH,Lu L,Zhao B.Automated Identification of Optimal Portal Venous Phase Timing with Convolutional Neural Networks.
2020;27:e10-e18 [PMID:31151901 DOI:10.1016/j.acra.2019.02.024]
34 Soomro MH,De Cola G,Conforto S,Schmid M,Giunta G,Guidi E,Neri E,Caruso D,Ciolina M,Laghi A.Automatic segmentation of colorectal cancer in 3D MRI by combining deep learning and 3D level-set algorithm-a preliminary study.2018 IEEE 4th middle east conference on biomedical engineering.2018:198-203 [DOI:10.1109/mecbme.2018.8402433]
35 Soomro MH,Coppotelli M,Conforto S,Schmid M,Giunta G,Del Secco L,Neri E,Caruso D,Rengo M,Laghi A.Automated Segmentation of Colorectal Tumor in 3D MRI Using 3D Multiscale Densely Connected Convolutional Neural Network.
2019;2019:1075434 [PMID:30838121 DOI:10.1155/2019/1075434]
36 Wang D,Xu J,Zhang Z,Li S,Zhang X,Zhou Y,Lu Y.Evaluation of Rectal Cancer Circumferential Resection Margin Using Faster Region-Based Convolutional Neural Network in High-Resolution Magnetic Resonance Images.
2020;63:143-151 [PMID:31842158 DOI:10.1097/DCR.0000000000001519]
37 Wu QY,Liu SL,Sun P,Li Y,Liu GW,Liu SS,Hu JL,Niu TY,Lu Y.Establishment and clinical application value of an automatic diagnosis platform for rectal cancer T-staging based on a deep neural network.
2021;134:821-828 [PMID:33797468 DOI:10.1097/CM9.0000000000001401]
38 Joshi N,Bond S,Brady M.The segmentation of colorectal MRI images.
2010;14:494-509 [PMID:20378393 DOI:10.1016/j.media.2010.03.002]
39 Dabass M,Vashisth S,Vig R.Review of classification techniques using deep learning for colorectal cancer imaging modalities.2019 6th International Conference on Signal Processing and Integrated Networks,2019 [DOI:10.1109/spin.2019.8711776]
40 Shiraishi T,Shinto E,Nearchou IP,Tsuda H,Kajiwara Y,Einama T,Caie PD,Kishi Y,Ueno H.Prognostic significance of mesothelin expression in colorectal cancer disclosed by area-specific fourpoint tissue microarrays.
2020;477:409-420 [PMID:32107600 DOI:10.1007/s00428-020-02775-y]
41 Pham TD.Scaling of texture in training autoencoders for classification of histological images of colorectal cancer.Advances in neural networks,2017:524-532 [DOI:10.1007/978-3-319-59081-3_61]
42 Tiwari S.An analysis in tissue classification for colorectal cancer histology using convolution neural network and colour models.
2018;9:1-19 [DOI:10.4018/ijismd.2018100101]
43 Sirinukunwattana K,Ahmed Raza SE,Yee-Wah Tsang,Snead DR,Cree IA,Rajpoot NM.Locality Sensitive Deep Learning for Detection and Classification of Nuclei in Routine Colon Cancer Histology Images.
2016;35:1196-1206 [PMID:26863654 DOI:10.1109/TMI.2016.2525803]
44 Koohababni NA,Jahanifar M,Gooya A,Rajpoot N.Nuclei detection using mixture density networks.Machine learning in medical imaging,2018:241-248 [DOI:10.1007/978-3-030-00919-9_28]
45 Zhang X,Chen G,Saruta K,Terata Y.An end-to-end cells detection approach for colon cancer histology images.10th international conference on digital image processing,2018 [DOI:10.1117/12.2503067]
46 Xu J,Luo X,Wang G,Gilmore H,Madabhushi A.A Deep Convolutional Neural Network for segmenting and classifying epithelial and stromal regions in histopathological images.
2016;191:214-223 [PMID:28154470 DOI:10.1016/j.neucom.2016.01.034]
47 Chen H,Qi X,Yu L,Dou Q,Qin J,Heng PA.DCAN:Deep contour-aware networks for object instance segmentation from histology images.
2017;36:135-146 [PMID:27898306 DOI:10.1016/j.media.2016.11.004]
48 Yoshida H,Yamashita Y,Shimazu T,Cosatto E,Kiyuna T,Taniguchi H,Sekine S,Ochiai A.Automated histological classification of whole slide images of colorectal biopsy specimens.
2017;8:90719-90729 [PMID:29207599 DOI:10.18632/oncotarget.21819]
49 Saito A,Cosatto E,Kiyuna T,Sakamoto M.Dawn of the digital diagnosis assisting system,can it open a new age for pathology? Medical imaging 2013:Digital pathology,2013 [DOI:10.1117/12.2008967]
50 Jin Y,Zhou C,Teng X,Ji J,Wu H,Liao J.Pai-wsit:An AI service platform with support for storing and sharing whole-slide images with metadata and annotations.
2019;7:54780-54786[DOI:10.1109/access.2019.2913255]
51 Qaiser T,Tsang YW,Taniyama D,Sakamoto N,Nakane K,Epstein D,Rajpoot N.Fast and accurate tumor segmentation of histology images using persistent homology and deep convolutional features.
2019;55:1-14 [PMID:30991188 DOI:10.1016/j.media.2019.03.014]
52 Chao WL,Manickavasagan H,Krishna SG.Application of Artificial Intelligence in the Detection and Differentiation of Colon Polyps:A Technical Review for Physicians.
2019;9 [PMID:31434208 DOI:10.3390/diagnostics9030099]
53 Zhou J,Wu L,Wan X,Shen L,Liu J,Zhang J,Jiang X,Wang Z,Yu S,Kang J,Li M,Hu S,Hu X,Gong D,Chen D,Yao L,Zhu Y,Yu H.A novel artificial intelligence system for the assessment of bowel preparation (with video).
2020;91:428-435.e2 [PMID:31783029 DOI:10.1016/j.gie.2019.11.026]
54 de Almeida Thomaz V,Sierra-Franco CA,Raposo AB.Training data enhancements for robust polyp segmentation in colonoscopy images.2019 IEEE 32nd International Symposium on Computer-Based Medical Systems (CBMS),2019:192-197 [DOI:10.1109/cbms.2019.00047]
55 Azer SA.Challenges Facing the Detection of Colonic Polyps:What Can Deep Learning Do?
2019;55 [PMID:31409050 DOI:10.3390/medicina55080473]
56 Taha B,Dias J,Werghi N,Ieee.Convolutional neural network as a feature extractor for automatic polyp detection.2017 24th IEEE international conference on image processing,2017:2060-2064[DOI:10.1109/icip.2017.8296644]
57 Yao H,Stidham RW,Soroushmehr R,Gryak J,Najarian K.Automated Detection of Non-Informative Frames for Colonoscopy Through a Combination of Deep Learning and Feature Extraction.
2019;2019:2402-2406 [PMID:31946383 DOI:10.1109/EMBC.2019.8856625]
58 McNeil MB,Gross SA.Siri here,cecum reached,but please wash that fold:Will artificial intelligence improve gastroenterology?
2020;91:425-427 [PMID:32036947 DOI:10.1016/j.gie.2019.10.027]
59 Bravo D,Ruano J,Gomez M,Romero E.Automatic detection of colorectal polyps larger than 5 mm during colonoscopy procedures using visual descriptors.14th international symposium on medical information processing and analysis,2018 [DOI:10.1117/12.2511577]
60 de Lange T,Halvorsen P,Riegler M.Methodology to develop machine learning algorithms to improve performance in gastrointestinal endoscopy.
2018;24:5057-5062[PMID:30568383 DOI:10.3748/wjg.v24.i45.5057]
61 Mahmood F,Durr NJ.Deep learning-based depth estimation from a synthetic endoscopy image training set.Medical imaging 2018:Image processing.Bellingham:Spie-Int Soc Optical Engineering,2018 [DOI:10.1117/12.2293785]
62 Mo X,Tao K,Wang Q,Wang G.An efficient approach for polyps detection in endoscopic videos based on faster R-CNN.2018 24th international conference on pattern recognition,2018:3929-3934[DOI:10.1109/icpr.2018.8545174]
63 Zhu H,Fan Y,Lu H,Liang Z.Improving initial polyp candidate extraction for CT colonography.
2010;55:2087-2102 [PMID:20299733 DOI:10.1088/0031-9155/55/7/019]
64 Komeda Y,Handa H,Watanabe T,Nomura T,Kitahashi M,Sakurai T,Okamoto A,Minami T,Kono M,Arizumi T,Takenaka M,Hagiwara S,Matsui S,Nishida N,Kashida H,Kudo M.Computer-Aided Diagnosis Based on Convolutional Neural Network System for Colorectal Polyp Classification:Preliminary Experience.
2017;93 Suppl 1:30-34 [PMID:29258081 DOI:10.1159/000481227]
65 Zhang R,Zheng Y,Poon CCY,Shen D,Lau JYW.Polyp detection during colonoscopy using a regression-based convolutional neural network with a tracker.
2018;83:209-219[PMID:31105338 DOI:10.1016/j.patcog.2018.05.026]
66 Zhu X,Nemoto D,Mizuno T,Nakajima Y,Utano K,Aizawa M,Takezawa T,Sagara Y,Hayashi Y,Katsuki S,Yamamoto H,Hewett DG,Togashi K.Identification of deeply invasive colorectal cancer on non-magnified endoscopic images using artificial intelligence.
2019;89
67 Akbari M,Mohrekesh M,Nasr-Esfahani E,Soroushmehr SMR,Karimi N,Samavi S,Najarian K.Polyp Segmentation in Colonoscopy Images Using Fully Convolutional Network.
2018;2018:69-72 [PMID:30440343 DOI:10.1109/EMBC.2018.8512197]
68 Lequan Yu,Hao Chen,Qi Dou,Jing Qin,Pheng Ann Heng.Integrating Online and Offline Three-Dimensional Deep Learning for Automated Polyp Detection in Colonoscopy Videos.
2017;21:65-75 [PMID:28114049 DOI:10.1109/JBHI.2016.2637004]
69 Yamada M,Saito Y,Imaoka H,Saiko M,Yamada S,Kondo H,Takamaru H,Sakamoto T,Sese J,Kuchiba A,Shibata T,Hamamoto R.Development of a real-time endoscopic image diagnosis support system using deep learning technology in colonoscopy.
2019;9:14465 [PMID:31594962 DOI:10.1038/s41598-019-50567-5]
70 Allescher HD,Weingart V.Optimizing Screening Colonoscopy:Strategies and Alternatives.
2019;35:215-225 [PMID:31602382 DOI:10.1159/000501835]
71 Lund Henriksen F,Jensen R,Kvale Stensland H,Johansen D,Riegler MA,Halvorsen P.Performance of data enhancements and training optimization for neural network:A polyp detection case study.2019 IEEE 32nd International Symposium on Computer-Based Medical Systems(CBMS),2019:287-293 [DOI:10.1109/cbms.2019.00067]
72 Ahmad OF,Soares AS,Mazomenos E,Brandao P,Vega R,Seward E,Stoyanov D,Chand M,Lovat LB.Artificial intelligence and computer-aided diagnosis in colonoscopy:current evidence and future directions.
2019;4:71-80 [PMID:30527583 DOI:10.1016/S2468-1253(18)30282-6]
73 Takamaru H,Wu SYS,Saito Y.Endocytoscopy:technology and clinical application in the lower GI tract.
2020;5:40 [PMID:32632391 DOI:10.21037/tgh.2019.12.04]
74 Rath T,Morgenstern N,Vitali F,Atreya R,Neurath MF.Advanced Endoscopic Imaging in Colonic Neoplasia.
2020;36:48-59 [PMID:32110657 DOI:10.1159/000505411]
75 Shahidi N,Rex DK,Kaltenbach T,Rastogi A,Ghalehjegh SH,Byrne MF.Use of Endoscopic Impression,Artificial Intelligence,and Pathologist Interpretation to Resolve Discrepancies Between Endoscopy and Pathology Analyses of Diminutive Colorectal Polyps.
2020;158:783-785.e1 [PMID:31863741 DOI:10.1053/j.gastro.2019.10.024]
76 Djinbachian R,Dubé AJ,von Renteln D.Optical Diagnosis of Colorectal Polyps:Recent Developments.
2019;17:99-114 [PMID:30746593 DOI:10.1007/s11938-019-00220-x]
77 Kudo SE,Misawa M,Mori Y,Hotta K,Ohtsuka K,Ikematsu H,Saito Y,Takeda K,Nakamura H,Ichimasa K,Ishigaki T,Toyoshima N,Kudo T,Hayashi T,Wakamura K,Baba T,Ishida F,Inoue H,Itoh H,Oda M,Mori K.Artificial Intelligence-assisted System Improves Endoscopic Identification of Colorectal Neoplasms.
2020;18:1874-1881.e2 [PMID:31525512 DOI:10.1016/j.cgh.2019.09.009]
78 Mahmood F,Durr NJ.Topographical reconstructions from monocular optical colonoscopy images via deep learning.2018 IEEE 15th international symposium on biomedical imaging,2018:216-219[DOI:10.1109/isbi.2018.8363558]
79 Vidyasagar M.Machine learning methods in the computational biology of cancer.
2014;470:20140081 [PMID:25002826 DOI:10.1016/j.arcontrol.2017.03.007]
80 Ebigbo A,Palm C,Probst A,Mendel R,Manzeneder J,Prinz F,de Souza LA,Papa JP,Siersema P,Messmann H.A technical review of artificial intelligence as applied to gastrointestinal endoscopy:clarifying the terminology.
2019;7:E1616-E1623 [PMID:31788542 DOI:10.1055/a-1010-5705]
81 Jian J,Xiong F,Xia W,Zhang R,Gu J,Wu X,Meng X,Gao X.Fully convolutional networks(FCNs)-based segmentation method for colorectal tumors on T2-weighted magnetic resonance images.
2018;41:393-401 [PMID:29654521 DOI:10.1007/s13246-018-0636-9]
82 Sivaganesan D.Wireless distributive personal communication for early detection of collateral cancer using optimized machine learning methodology.
2016;94:2291-2302 [DOI:10.1007/s11277-016-3411-9]
83 Gayathri Devi K,Radhakrishnan R.Automatic segmentation of colon in 3D CT images and removal of opacified fluid using cascade feed forward neural network.
2015;2015:670739 [PMID:25838838 DOI:10.1155/2015/670739]
84 Therrien R,Doyle S.Role of training data variability on classifier performance and generalizability.Medical imaging 2018:Digital pathology,2018 [DOI:10.1117/12.2293919]
85 Sun CY,Liu W,Doyle S.Two-tier classifier for identifying small objects in histological tissue classification:Experiments with colon cancer tissue mapping.Medical imaging 2019:Digital pathology,2019 [DOI:10.1117/12.2512973]
86 Shi J,Su Q,Zhang C,Huang G,Zhu Y.An intelligent decision support algorithm for diagnosis of colorectal cancer through serum tumor markers.
2010;100:97-107 [PMID:20346535 DOI:10.1016/j.cmpb.2010.03.001]
87 Su Q,Shi J,Gu P,Huang G,Zhu Y.An algorithm designed for improving diagnostic efficiency by setting multi-cutoff values of multiple tumor markers.
2012;39:5784-5791 [DOI:10.1016/j.eswa.2011.11.089]
88 Kunhoth S,Al Maadeed S.Building a multispectral image dataset for colorectal tumor biopsy.2017 13th international wireless communications and mobile computing conference,2017:1745-1750 [DOI:10.1109/iwcmc.2017.7986548]
89 Wang P,Xiao X,Glissen Brown JR,Berzin TM,Tu M,Xiong F,Hu X,Liu P,Song Y,Zhang D,Yang X,Li L,He J,Yi X,Liu J,Liu X.Development and validation of a deep-learning algorithm for the detection of polyps during colonoscopy.
2018;2:741-748 [PMID:31015647 DOI:10.1038/s41551-018-0301-3]
90 Barua I,Vinsard DG,Jodal HC,L?berg M,Kalager M,Holme ?,Misawa M,Bretthauer M,Mori Y.Artificial intelligence for polyp detection during colonoscopy:a systematic review and metaanalysis.
2021;53:277-284 [PMID:32557490 DOI:10.1055/a-1201-7165]
91 Gong D,Wu L,Zhang J,Mu G,Shen L,Liu J,Wang Z,Zhou W,An P,Huang X,Jiang X,Li Y,Wan X,Hu S,Chen Y,Hu X,Xu Y,Zhu X,Li S,Yao L,He X,Chen D,Huang L,Wei X,Wang X,Yu H.Detection of colorectal adenomas with a real-time computer-aided system (ENDOANGEL):a randomised controlled study.
2020;5:352-361 [PMID:31981518 DOI:10.1016/S2468-1253(19)30413-3]
92 Lui TKL,Leung WK.Is artificial intelligence the final answer to missed polyps in colonoscopy?
2020;26:5248-5255 [PMID:32994685 DOI:10.3748/wjg.v26.i35.5248]
93 Rodriguez-Diaz E,Castanon DA,Singh SK,Bigio IJ.Spectral classifier design with ensemble classifiers and misclassification-rejection:application to elastic-scattering spectroscopy for detection of colonic neoplasia.
2011;16:067009 [PMID:21721830 DOI:10.1117/1.3592488]
94 Kondepati VR,Oszinda T,Heise HM,Luig K,Mueller R,Schroeder O,Keese M,Backhaus J.CHovertone regions as diagnostic markers for near-infrared spectroscopic diagnosis of primary cancers in human pancreas and colorectal tissue.
2007;387:1633-1641 [PMID:17205263 DOI:10.1007/s00216-006-0960-x]
95 Angermann Q,Histace A,Romain O.Active learning for real time detection of polyps in videocolonoscopy.20th conference on medical image understanding and analysis,2016:182-187[DOI:10.1016/j.procs.2016.07.017]
96 Ayling RM,Lewis SJ,Cotter F.Potential roles of artificial intelligence learning and faecal immunochemical testing for prioritisation of colonoscopy in anaemia.
2019;185:311-316 [PMID:30714125 DOI:10.1111/bjh.15776]
97 Tian X,Xu LL,Liu XL,Chen WQ.Enhanced Patient Education for Colonic Polyp and Adenoma Detection:Meta-Analysis of Randomized Controlled Trials.
2020;8:e17372[PMID:32347798 DOI:10.2196/17372]
98 Javed S,Fraz MM,Epstein D,Snead D,Rajpoot NM.Cellular community detection for tissue phenotyping in histology images.Computational pathology and ophthalmic medical image analysis,2018:120-129 [DOI:10.1007/978-3-030-00949-6_15]
99 Wang Q,Wei J,Chen Z,Zhang T,Zhong J,Zhong B,Yang P,Li W,Cao J.Establishment of multiple diagnosis models for colorectal cancer with artificial neural networks.
2019;17:3314-3322 [PMID:30867765 DOI:10.3892/ol.2019.10010]
100 Battista A,Battista RA,Battista F,Cinquanta L,Iovane G,Corbisieri M,Suozzo A.Development of a new mathematical tool for early colorectal cancer diagnosis and its possible use in mass screening.
2019;22:811-835 [DOI:10.1080/09720502.2019.1649834]
101 Zhang W,Chen X,Wong KC.Noninvasive early diagnosis of intestinal diseases based on artificial intelligence in genomics and microbiome.
2021;36:823-831 [PMID:33880763 DOI:10.1111/jgh.15500]
102 Wang KS,Yu G,Xu C,Meng XH,Zhou J,Zheng C,Deng Z,Shang L,Liu R,Su S,Zhou X,Li Q,Li J,Wang J,Ma K,Qi J,Hu Z,Tang P,Deng J,Qiu X,Li BY,Shen WD,Quan RP,Yang JT,Huang LY,Xiao Y,Yang ZC,Li Z,Wang SC,Ren H,Liang C,Guo W,Li Y,Xiao H,Gu Y,Yun JP,Huang D,Song Z,Fan X,Chen L,Yan X,Huang ZC,Huang J,Luttrell J,Zhang CY,Zhou W,Zhang K,Yi C,Wu C,Shen H,Wang YP,Xiao HM,Deng HW.Accurate diagnosis of colorectal cancer based on histopathology images using artificial intelligence.
2021;19:76 [PMID:33752648 DOI:10.1186/s12916-021-01942-5]
103 Jones OT,Calanzani N,Saji S,Duffy SW,Emery J,Hamilton W,Singh H,de Wit NJ,Walter FM.Artificial Intelligence Techniques That May Be Applied to Primary Care Data to Facilitate Earlier Diagnosis of Cancer:Systematic Review.
2021;23:e23483 [PMID:33656443 DOI:10.2196/23483]
104 Lorenzovici N,Dulf EH,Mocan T,Mocan L.Artificial Intelligence in Colorectal Cancer Diagnosis Using Clinical Data:Non-Invasive Approach.
2021;11 [PMID:33799452 DOI:10.3390/diagnostics11030514]
105 Xu Y,Ding W,Wang Y,Tan Y,Xi C,Ye N,Wu D,Xu X.Comparison of diagnostic performance between convolutional neural networks and human endoscopists for diagnosis of colorectal polyp:A systematic review and meta-analysis.
2021;16:e0246892 [PMID:33592048 DOI:10.1371/journal.pone.0246892]
106 ?ztürk ?,?zkaya U.Residual LSTM layered CNN for classification of gastrointestinal tract diseases.
2021;113:103638 [PMID:33271341 DOI:10.1016/j.jbi.2020.103638]
107 Echle A,Rindtorff NT,Brinker TJ,Luedde T,Pearson AT,Kather JN.Deep learning in cancer pathology:a new generation of clinical biomarkers.
2021;124:686-696 [PMID:33204028 DOI:10.1038/s41416-020-01122-x]
108 Araujo RL,Linhares MM.Pushing the limits of liver surgery for colorectal liver metastases:Current state and future directions.
2019;11:34-40 [PMID:30842810 DOI:10.4240/wjgs.v11.i2.34]
109 Passi K,Zhao H.A decision support system (DSS) for colorectal cancer follow-up program
a semantic framework.
2015;10:17-38 [DOI:10.4018/ijhisi.2015010102]
110 Lee WS,Ahn SM,Chung JW,Kim KO,Kwon KA,Kim Y,Sym S,Shin D,Park I,Lee U,Baek JH.Assessing Concordance With Watson for Oncology,a Cognitive Computing Decision Support System for Colon Cancer Treatment in Korea.
2018;2:1-8 [PMID:30652564 DOI:10.1200/CCI.17.00109]
111 Siddiqi J,Akhgar B,Gruzdz A,Zaefarian G,Ihnatowicz A.Automated diagnosis system to support colon cancer treatment:Match.15th International Conference on Information Technology:New Generations,2008:201-205 [DOI:10.1109/itng.2008.62]
112 Li S,Jiang Q,Liu S,Zhang Y,Tian Y,Song C,Wang J,Zou Y,Anderson GJ,Han JY,Chang Y,Liu Y,Zhang C,Chen L,Zhou G,Nie G,Yan H,Ding B,Zhao Y.A DNA nanorobot functions as a cancer therapeutic in response to a molecular trigger in vivo.
2018;36:258-264[PMID:29431737 DOI:10.1038/nbt.4071]
113 Felfoul O,Mohammadi M,Taherkhani S,de Lanauze D,Zhong Xu Y,Loghin D,Essa S,Jancik S,Houle D,Lafleur M,Gaboury L,Tabrizian M,Kaou N,Atkin M,Vuong T,Batist G,Beauchemin N,Radzioch D,Martel S.Magneto-aerotactic bacteria deliver drug-containing nanoliposomes to tumour hypoxic regions.
2016;11:941-947 [PMID:27525475 DOI:10.1038/nnano.2016.137]
114 Koelzer VH,Sirinukunwattana K,Rittscher J,Mertz KD.Precision immunoprofiling by image analysis and artificial intelligence.
2019;474:511-522 [PMID:30470933 DOI:10.1007/s00428-018-2485-z]
115 Dzobo K,Thomford NE,Senthebane DA.Targeting the Versatile Wnt/β-Catenin Pathway in Cancer Biology and Therapeutics:From Concept to Actionable Strategy.
2019;23:517-538 [PMID:31613700 DOI:10.1089/omi.2019.0147]
116 Lee BI,Matsuda T.Estimation of Invasion Depth:The First Key to Successful Colorectal ESD.
2019;52:100-106 [PMID:30914629 DOI:10.5946/ce.2019.012]
117 Ichimasa K,Kudo SE,Mori Y,Misawa M,Matsudaira S,Kouyama Y,Baba T,Hidaka E,Wakamura K,Hayashi T,Kudo T,Ishigaki T,Yagawa Y,Nakamura H,Takeda K,Haji A,Hamatani S,Mori K,Ishida F,Miyachi H.Artificial intelligence may help in predicting the need for additional surgery after endoscopic resection of T1 colorectal cancer.
2018;50:230-240[PMID:29272905 DOI:10.1055/s-0043-122385]
118 Kirchberg J,Weitz J.Evidence for robotic surgery in oncological visceral surgery.
2019;90:379-386 [PMID:30778607 DOI:10.1007/s00104-019-0812-9]
119 Kim YJ.The Future Medical Science and Colorectal Surgeons.
2017;33:207-209[PMID:29354602 DOI:10.3393/ac.2017.33.6.207]
120 Leonard S,Wu KL,Kim Y,Krieger A,Kim PC.Smart tissue anastomosis robot (STAR):a visionguided robotics system for laparoscopic suturing.
2014;61:1305-1317[PMID:24658254 DOI:10.1109/TBME.2014.2302385]
121 Huang YM,Huang YJ,Wei PL.Colorectal Cancer Surgery Using the Da Vinci Xi and Si Systems:Comparison of Perioperative Outcomes.
2019;26:192-200 [PMID:30501567 DOI:10.1177/1553350618816788]
122 Zheng P,Feng QY,Xu JM.Current status and consideration of robotic surgery for colorectal cancer in China.
2020;23:336-340 [PMID:32306599 DOI:10.3760/cma.j.cn.441530-20200216-00056]
123 Mitsala A,Tsalikidis C,Pitiakoudis M,Simopoulos C,Tsaroucha AK.Artificial Intelligence in Colorectal Cancer Screening,Diagnosis and Treatment.A New Era.
2021;28:1581-1607 [PMID:33922402 DOI:10.3390/curroncol28030149]
124 Aikemu B,Xue P,Hong H,Jia H,Wang C,Li S,Huang L,Ding X,Zhang H,Cai G,Lu A,Xie L,Li H,Zheng M,Sun J.Artificial Intelligence in Decision-Making for Colorectal Cancer Treatment Strategy:An Observational Study of Implementing Watson for Oncology in a 250-Case Cohort.
2020;10:594182 [PMID:33628729 DOI:10.3389/fonc.2020.594182]
125 Hamamoto R,Suvarna K,Yamada M,Kobayashi K,Shinkai N,Miyake M,Takahashi M,Jinnai S,Shimoyama R,Sakai A,Takasawa K,Bolatkan A,Shozu K,Dozen A,Machino H,Takahashi S,Asada K,Komatsu M,Sese J,Kaneko S.Application of Artificial Intelligence Technology in Oncology:Towards the Establishment of Precision Medicine.
2020;12 [PMID:33256107 DOI:10.3390/cancers12123532]
126 Pritzker KPH.Colon Cancer Biomarkers:Implications for Personalized Medicine.
2020;10 [PMID:33066312 DOI:10.3390/jpm10040167]
127 Ding X,Chang VHS,Li Y,Li X,Xu H,Ho C-M,Ho D,Yen Y.Harnessing an artificial intelligence platform to dynamically individualize combination therapy for treating colorectal carcinoma in a rat model.
2020;3 [DOI:10.1002/adtp.201900127]
128 Zhang L,Zheng C,Li T,Xing L,Zeng H,Yang H,Cao J,Chen B,Zhou Z.Building up a robust risk mathematical platform to predict colorectal cancer.
2017;2017:1-14 [DOI:10.1155/2017/8917258]
129 Morgado P,Vicente H,Abelha A,Machado J,Neves J.A case-based approach to colorectal cancer detection.Information science and applications,2017:433-442 [DOI:10.1007/978-981-10-4154-9_50]
130 Cueto-López N,García-Ordás MT,Dávila-Batista V,Moreno V,Aragonés N,Alaiz-Rodríguez R.A comparative study on feature selection for a risk prediction model for colorectal cancer.
2019;177:219-229 [PMID:31319951 DOI:10.1016/j.cmpb.2019.06.001]
131 Anand SS,Smith AE,Hamilton PW,Anand JS,Hughes JG,Bartels PH.An evaluation of intelligent prognostic systems for colorectal cancer.
1999;15:193-214 [PMID:10082181 DOI:10.1016/s0933-3657(98)00052-9]
132 Gupta P,Chiang SF,Sahoo PK,Mohapatra SK,You JF,Onthoni DD,Hung HY,Chiang JM,Huang Y,Tsai WS.Prediction of Colon Cancer Stages and Survival Period with Machine Learning Approach.
2019;11 [PMID:31842486 DOI:10.3390/cancers11122007]
133 Li S,Razzaghi T.Personalized colorectal cancer survivability prediction with machine learning methods.2018 IEEE international conference on big data,2018:2554-2558 [DOI:10.1109/bigdata.2018.8622121]
134 Barsainya A,Sairam A,Patil AP.Analysis and prediction of survival after colorectal chemotherapy using machine learning models.2018 International Conference on Advances in Computing,Communications and Informatics,2018 [DOI:10.1109/icacci.2018.8554832]
135 Dimitriou N,Arandjelovi? O,Harrison DJ,Caie PD.A principled machine learning framework improves accuracy of stage II colorectal cancer prognosis.
2018;1:52 [PMID:31304331 DOI:10.1038/s41746-018-0057-x]
136 Popovici V,Budinská E,Du?ek L,Kozubek M,Bosman F.Image-based surrogate biomarkers for molecular subtypes of colorectal cancer.
2017;33:2002-2009 [PMID:28158480 DOI:10.1093/bioinformatics/btx027]
137 Hoogendoorn M,Szolovits P,Moons LMG,Numans ME.Utilizing uncoded consultation notes from electronic medical records for predictive modeling of colorectal cancer.
2016;69:53-61 [PMID:27085847 DOI:10.1016/j.artmed.2016.03.003]
138 Kop R,Hoogendoorn M,Teije AT,Büchner FL,Slottje P,Moons LM,Numans ME.Predictive modeling of colorectal cancer using a dedicated pre-processing pipeline on routine electronic medical records.
2016;76:30-38 [PMID:27392227 DOI:10.1016/j.compbiomed.2016.06.019]
139 Geessink OGF,Baidoshvili A,Freling G,Klaase JM,Slump CH,van der Heijden F.Toward automatic segmentation and quantification of tumor and stroma in whole-slide images of H&E stained rectal carcinomas.Medical imaging 2015:Digital pathology.Bellingham:Spie-Int Soc Optical Engineering,2015 [DOI:10.1117/12.2081665]
140 Wright A,Magee D,Quirke P,Treanor D.Towards automatic patient selection for chemotherapy in colorectal cancer trials.Medical imaging 2014:Digital pathology,2014 [DOI:10.1117/12.2043220]
141 Wang Y,Wang D,Ye X,Wang Y,Yin Y,Jin Y.A tree ensemble-based two-stage model for advanced-stage colorectal cancer survival prediction.
2019;474:106-124 [DOI:10.1016/j.ins.2018.09.046]
142 Oliveira T,Barbosa E,Martins S,Goulart A,Neves J,Novais P.A prognosis system for colorectal cancer.Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems,2013 [DOI:10.1109/cbms.2013.6627846]
143 Lo Bello L,Pistone G,Restuccia S,Vinci E,Mazzoleni G,Malaguarnera M.5-fluorouracil alone versus 5-fluorouracil plus folinic acid in the treatment of colorectal carcinoma:meta-analysis.
2000;38:553-562 [PMID:11125868 DOI:10.5414/cpp38553]
144 Harrington L,Suriawinata A,MacKenzie T,Hassanpour S.Application of machine learning on colonoscopy screening records for predicting colorectal polyp recurrence.Proceedings 2018 IEEE international conference on bioinformatics and biomedicine,2018:993-998 [DOI:10.1109/bibm.2018.8621455]
145 Xie X,Xing J,Kong N,Li C,Li J,Zhang S.Improving colorectal polyp classification based on physical examination data-an ensemble learning approach.
2018;3:434-441 [DOI:10.1109/lra.2017.2746918]
146 Bokhorst JM,Rijstenberg L,Goudkade D,Nagtegaal I,van der Laak J,Ciompi F.Automatic detection of tumor budding in colorectal carcinoma with deep learning.Computational pathology and ophthalmic medical image analysis,2018:130-138 [DOI:10.1007/978-3-030-00949-6_16]
147 Zhao K,Li Z,Yao S,Wang Y,Wu X,Xu Z,Wu L,Huang Y,Liang C,Liu Z.Artificial intelligence quantified tumour-stroma ratio is an independent predictor for overall survival in resectable colorectal cancer.
2020;61:103054 [PMID:33039706 DOI:10.1016/j.ebiom.2020.103054]
148 Syafiandini AF,Wasito I,Yazid S,Fitriawan A,Amien M.Cancer subtype identification using deep learning approach.2016 International Conference on Computer,Control,Informatics and its Applications,2016 [DOI:10.1109/ic3ina.2016.7863033]
149 Roadknight C,Aickelin U,Scholefield J,Durrant L.Ensemble learning of colorectal cancer survival rates.2013 IEEE international conference on computational intelligence and virtual environments for measurement systems and applications,2013:82-86 [DOI:10.1109/civemsa.2013.6617400]
150 Cui Y,Cai X,Jin Z.Semi-supervised classification using sparse representation for cancer recurrence prediction.2013 IEEE international workshop on genomic signal processing and statistics,2013:102-105 [DOI:10.1109/gensips.2013.6735949]
151 Park C,Ahn J,Kim H,Park S.Integrative gene network construction to analyze cancer recurrence using semi-supervised learning.
2014;9:e86309 [PMID:24497942 DOI:10.1371/journal.pone.0086309]
152 Du X,Cheng J.Identification and analysis of driver missense mutations using rotation forest with feature selection.
2014;2014:905951 [PMID:25250338 DOI:10.1155/2014/905951]
153 Chi S,Li X,Tian Y,Li J,Kong X,Ding K,Weng C.Semi-supervised learning to improve generalizability of risk prediction models.
2019;92:103117 [PMID:30738948 DOI:10.1016/j.jbi.2019.103117]
154 Ong LS,Shepherd B,Tong LC,Seow-Choen F,Ho YH,Tang CL,Ho YS,Tan K.The Colorectal Cancer Recurrence Support (CARES) System.
1997;11:175-188 [PMID:9413605 DOI:10.1016/s0933-3657(97)00029-8]
155 Reichling C,Taieb J,Derangere V,Klopfenstein Q,Le Malicot K,Gornet JM,Becheur H,Fein F,Cojocarasu O,Kaminsky MC,Lagasse JP,Luet D,Nguyen S,Etienne PL,Gasmi M,Vanoli A,Perrier H,Puig PL,Emile JF,Lepage C,Ghiringhelli F.Artificial intelligence-guided tissue analysis combined with immune infiltrate assessment predicts stage III colon cancer outcomes in PETACC08 study.
2020;69:681-690 [PMID:31780575 DOI:10.1136/gutjnl-2019-319292]
156 Chowdhury SA,Nibbe RK,Chance MR,Koyutürk M.Subnetwork state functions define dysregulated subnetworks in cancer.
2011;18:263-281 [PMID:21385033 DOI:10.1089/cmb.2010.0269]
157 Mohamad Marzuki MF,Yaacob NA,Bin Yaacob NM,Abu Hassan MR,Ahmad SB.Usable Mobile App for Community Education on Colorectal Cancer:Development Process and Usability Study.
2019;6:e12103 [PMID:30990454 DOI:10.2196/12103]
158 Hacking S,Nasim R,Lee L,Vitkovski T,Thomas R,Shaffer E,Nasim M.Whole slide imaging and colorectal carcinoma:A validation study for tumor budding and stromal differentiation.
2020;216:153233 [PMID:33068916 DOI:10.1016/j.prp.2020.153233]
159 Wang Y,He X,Nie H,Zhou J,Cao P,Ou C.Application of artificial intelligence to the diagnosis and therapy of colorectal cancer.
2020;10:3575-3598 [PMID:33294256]
160 O'Sullivan S,Nevejans N,Allen C,Blyth A,Leonard S,Pagallo U,Holzinger K,Holzinger A,Sajid MI,Ashrafian H.Legal,regulatory,and ethical frameworks for development of standards in artificial intelligence (AI) and autonomous robotic surgery.
2019;15:e1968 [PMID:30397993 DOI:10.1002/rcs.1968]
 World Journal of Gastrointestinal Oncology2022年1期
World Journal of Gastrointestinal Oncology2022年1期
- World Journal of Gastrointestinal Oncology的其它文章
- Comment on “Outcomes of curative liver resection for hepatocellular carcinoma in patients with cirrhosis”
- Liquid biopsy:Precise diagnosis and therapy for cholangiocarcinoma
- Increased risk of colorectal neoplasia in inflammatory bowel disease patients with post-inflammatory polyps:A systematic review and meta-analysis
- Exosomes as potential diagnosis and treatment for liver cancer
- Effects of cognitive behavior therapy combined with Baduanjin in patients with colorectal cancer
- Intertwined leukocyte balances in tumours and peripheral blood as robust predictors of right and left colorectal cancer survival