
Statin as a therapeutic agent in gastroenterological cancer
2022-01-25 02:55:26NorioUemuraHiromitsuHayashiHideoBaba
INTRODUCTION
Since the clinical application of statins in the late 1980s,statins have dramatically improved the clinical management of high cholesterol and ischemic heart disease,and their use has become widespread worldwide.Statins are specified inhibitors of the mevalonate (MVA) pathway,that is involved in thesynthesis of cholesterol and other nonsterol isoprenoids.The rate-limiting enzyme in MVA synthesis is 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMGCR)[1,2].Statins function by inhibiting HMGCR and are effective in the management of hypercholesterolemia.
In addition to their functional role in normal physiology,the MVA pathway is noted to support tumorigenesis and be dysregulated in cancers[3-5].The MVA pathway is a vital metabolic pathway that uses acetyl-CoA to generate isoprenoids and sterols,which are crucial to tumor growth and progression.Therefore,there is a great deal of interest in repurposing statins as anticancer drugs.Numerous cohort studies have announced that statin use is linked with lower risk of cancer development,lower cancer grade at diagnosis,and lower recurrence and cancer-related death[6].Several randomized clinical trials have investigated the advantages of adding statins to anticancer agents.However,most of the trials did not show an improvement in prognosis and have not led to the clinical application of statins.The development of new anticancer drugs is progressing but increasing medical costs from drug development have become a major obstacle.Readily available,inexpensive and well-tolerated drugs like statins have not yet been successfully repurposed for cancer treatment.Planning clinical trials is difficult,and it is possible that the previous clinical trials were poorly designed[7].In the age of precision medicine,defining the cancer patients that may benefit from statins is critical.
At length, in the afternoon, the old woman noticed this particular nanny-goat stealing off by herself away from the herd10 and she at once went after her
This review summarizes the results of recent basic research and clinical studies on statins in cancer and suggests strategies for future clinical trial planning.In addition,the potential for the clinical application of statins in cancer treatment is discussed.
MECHANISMS OF ACTION OF STATINS
The MVA pathway is a vital metabolic pathway that uses acetyl-CoA to generate isoprenoids and sterols,which are crucial to tumor growth and progression.In the first step of the MVA pathway,the rate-limiting enzyme HMGCR converts HMG-CoA to MVA (Figure 1).MVA is further metabolized to farnesyl pyrophosphate (FPP).FPP is the precursor in cholesterol and steroid biosynthesis as well as in the biosynthesis of dolichols.Intracellular cholesterol preserves sterol regulatory element-binding proteins (SREBPs) as an inactive form in their full-length.In a situation of cholesterol depletion,SREBP proteins are cleaved,releasing the active transcription factors involved in the MVA pathway and cholesterol transport.
So the Herd-boy went back to his hut, and taking his loaf and belt with him, he went to the nearest town. There he bought himself some fine clothes, and a beautiful coach with four horses, hired two servants, and drove back to his master. You may imagine how astonished he was to see his Herd-boy returning to him in this manner! Then the youth told him of the piece of good luck that had befallen him, and asked him for the hand of his beautiful daughter. This was readily granted, and the two lived in peace and happiness to the end of their lives.

Statins bind to the active site of HMGCR,compete with HMG-CoA,and reduce MVA synthesis.Hence,statins exhaust intracellular cholesterol,causing a homeostatic feedback machinery by the SREBP family of transcription factors.Activation of SREBPs increases the gene expression of low density lipoprotein (LDL) receptor(LDLR).Increased membrane expression of LDLR promotes the uptake of LDL cholesterol from the blood circulation and efficiently lowers serum cholesterol levels.Statins are generally prescribed to lower blood cholesterol,decrease the risk of cardiovascular disease,or enhance the survival rate of cases with cardiovascular disease.
MVA PATHWAY IN CANCER
The MVA pathway has been shown to play a multifaceted role in tumorigenesis[4,8].The PI3K/AKT pathway is a critical regulator of cell proliferation and cell survival in response to growth factors.PI3K/AKT signaling activates the MVA pathway through increasing the expression of SREBPs.The increase in lipid and cholesterol generation regulated by the PI3K/AKT/SREBPs axis enhances the tumorigenesis and cancer growth[9,10].Conversely,inhibition of the MVA pathway decreases PI3K activity through decreased RAS isoprenylation[11].
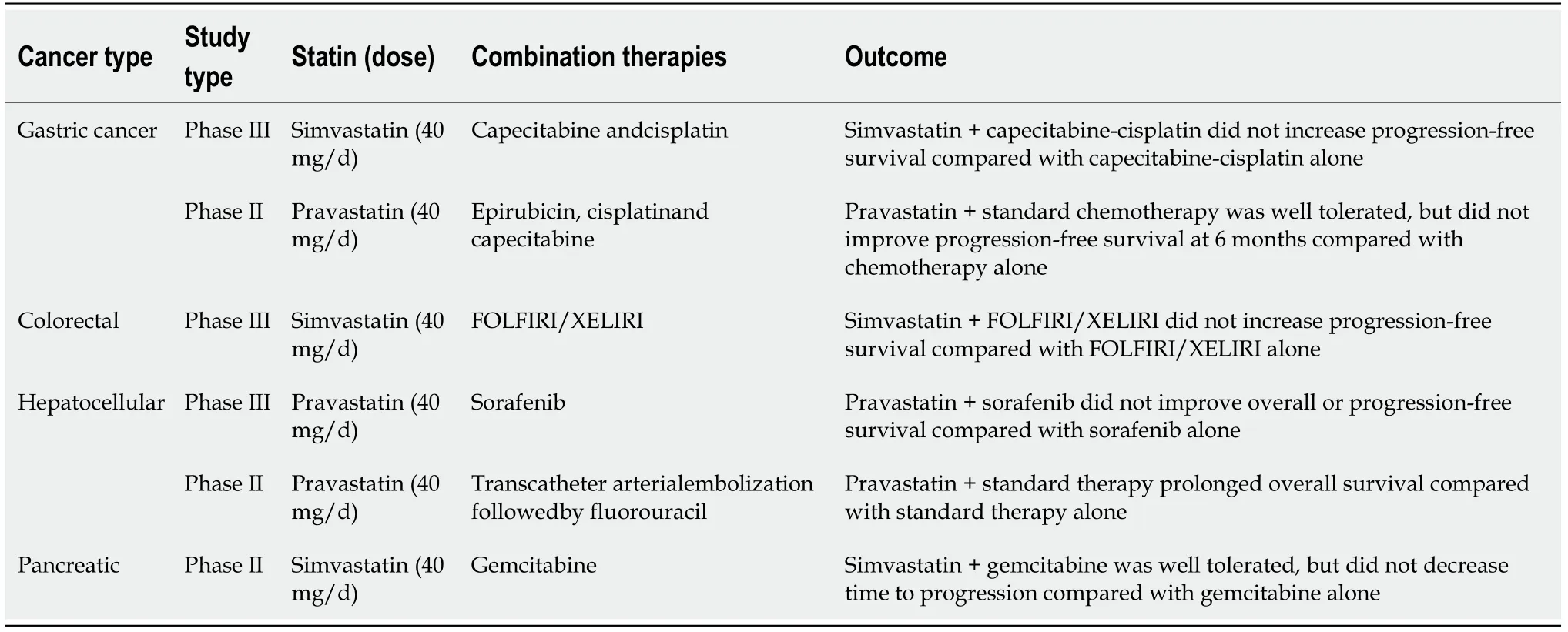
Previous RCTs used simvastatin and pravastatin at 40 mg/d,which are moderateintensity prescriptions (Table 1),and therefore higher doses or prescription of a higher-intensity statin might have provided enhanced responses in these studies.Drug combination strategies to reinforce the anti-cancer effect of statins should also be evaluated for future RCTs.
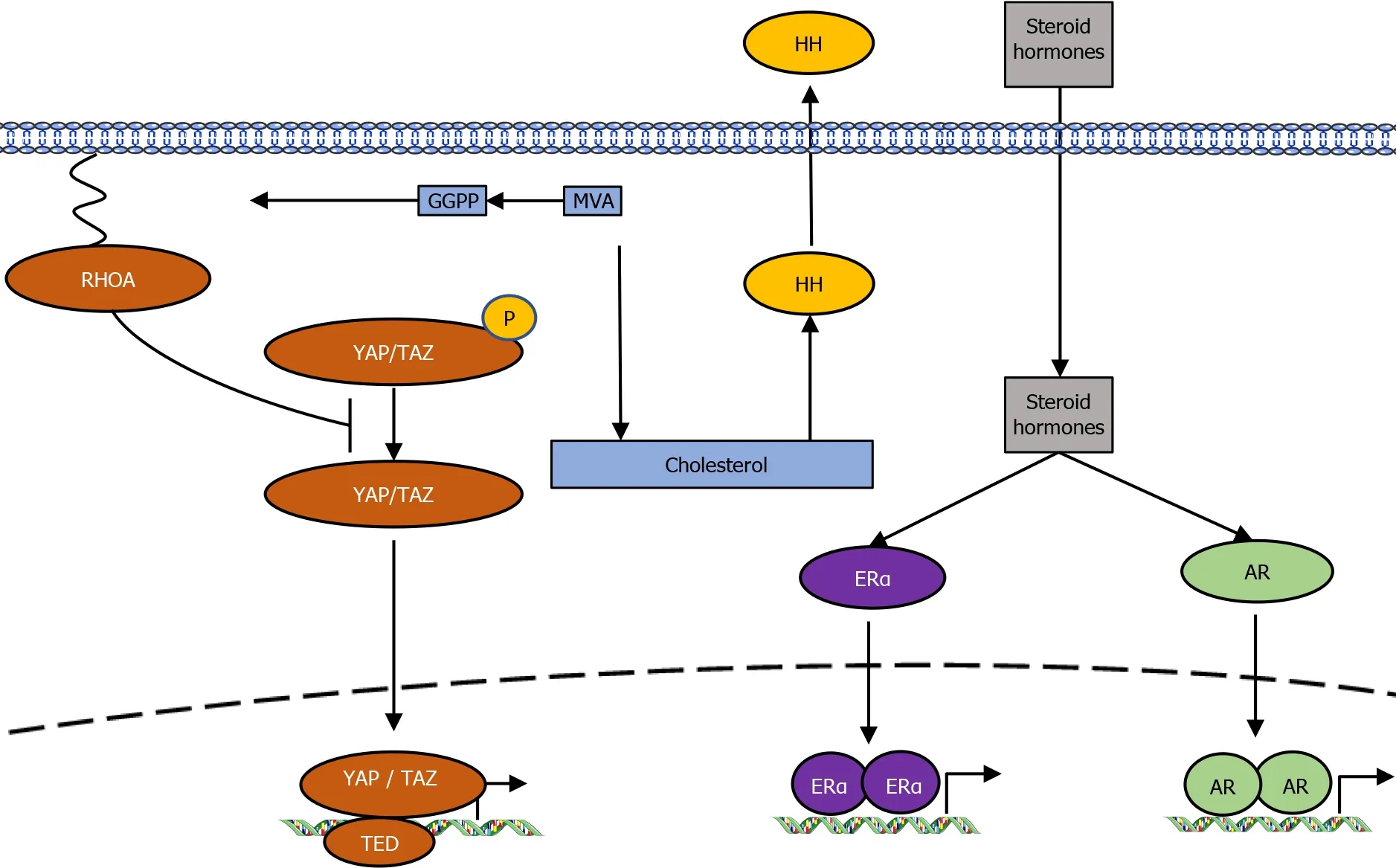
The Hedgehog (HH) signaling pathway,which has crucial roles in tumorigenesis,is controlled by cholesterol.Cholesterol and cholesterol-derived oxysterols activate HH signal transduction[17],whereas inhibition of the MVA pathway or downstream sterol biosynthesis decreases HH signaling and reduces cell proliferation.
Cholesterol is the precursor for steroid hormones such as estrogen and androgen.These hormones are implicated in hormone-driven breast cancers and prostate cancersthe activation of estrogen receptor-α (ERα) and androgen receptor,respectively[18,19].Perhaps because of these functions,research into the antitumor effects of statins is the most advanced in the fields of breast cancer,ovarian cancer,and prostate cancer.
Bill was a retired, life long bachelor. He lived alone in the small terraced house() next door but two from us. On a number of occasions, I visited Bill s house, and it seemed that it hadn t really changed much from the 50s. There were hints that some articles had been undisturbed apart from the occasional silverfish or visiting woodlouse, since the 1930s.
The members of the SREBP family of transcription factors control the upregulation ofand other lipid metabolism genes and are activated to restore homeostasis in response to cholesterol depletion (Figure 1).A subset of cell lines and primary cells from multiple myeloma patients were unable to provoke the expression of SREBP target genes by statin treatment and readily undergo apoptosis[64].On the contrary,cell lines with potent statin-induced activation of SREBPs were resistive to statin treatment.In prostate cancer,this sterol-regulated feedback loop may modulate statin sensitivity,and a combination therapy of statins and SREBP inhibitors has a synergistic effect in prostate cancer[65].Although it is theoretically convincing that feedback dysregulation of the MVA pathway is involved in statin sensitivity,further research is required to verify whether SREBPs can be clinically useful biomarkers.
STATINS AND ESOPHAGEAL CANCER
Three meta-analyses have been conducted on the effects of statins on esophageal cancer.In a meta-analysis of five cohort studies comprising 24576 patients,Zhou[21] reported that statin use in esophageal cancer patients was associated with a 26%improved overall survival [OS;95% confidence interval (CI):0.75–0.94] and diseasefree survival (95%CI:0.75–0.96)[22-26].Deng[27] reported that statin use was considerably associated with decreased all-cause [random effects:Hazard ratio (HR)=0.81,95%CI:0.75–0.89,<0.001] and cancer-specific mortality (fixed effects:HR=0.84,95%CI:0.78–0.89,<0.001) in esophageal cancer from four cohort studies involving a total of 20435 patients[25].In the subgroup analysis,both meta-analyses showed an effect of statins on improving prognosis regardless of the histological type of squamous cell carcinoma and adenocarcinoma.Thomas[28] insisted that statins might play a protective role against esophageal cancer development in cases with or without Barrett’s esophagus.
STATINS AND GASTRIC CANCER
Two randomized controlled trials (RCTs) have examined the effects of statin combination therapy on gastric cancer.A phase III study that examined simvastatin(40 mg/d) plus capecitabine-cisplatin compared with capecitabin-cisplatin alone did not show increased progression-free survival[29].A phase II study that examined pravastatin (40 mg/d) plus standard chemotherapy revealed no improvement of the progression-free survival rate at 6 mo compared with standard chemotherapy alone[30].A matched case-control study reported that statin use in patients who underwent radical gastrectomy for stage II and III gastric cancer was associated with good prognosis.No significant differences were shown in relapse-free survival or OS between statin users and non-users.On the other hand,subgroup analysis revealed that patients who used statins for more than 6 mo showed better prognostic outcomes than non-users or those who used statins for less than 6 mo[31].A population-based cohort study including 3833 patients with gastric cancer showed that statin use was linked with decreased cancer-specific mortality (adjusted HR=0.83,95%CI:0.74–0.92)[32].Several studies have shown that the use of statins reduces the risk of gastric cancer[33-35].
STATINS AND COLORECTAL CANCER
Many epidemiologic and clinical studies have been performed on statins and colorectal cancer (CRC).However,the results have been inconsistent.One notable observational study from Israel showed that 5 or more years of statin use was linked with a 45% decrease in CRC risk (95%CI:0.40–0.74)[36].An another study of United States veterans also revealed a 35% decrease in CRC risk with statin use (95%CI:0.55–0.78)[37].On the other hand,several meta-analyses of case-control and cohort studies have revealed smaller risk decreases[38,39],or no relationship[40,41].The unconvincing results from observational studies could be due to healthier behaviors in statin users compared with nonusers,the different durations of statin intake[39],different hydrophilicity of specific statins[42],or different effects of statins on colon or rectal cancers[43,44].
STATINS AND HEPATOCELLULAR CARCINOMA
A nationwide population-based nested case-control study of patients with diabetes indicated a dose-dependent reduction of hepatocellular carcinoma (HCC) incidence with statin treatment[45].In this study,statin users had a dose-dependent [cumulative defined daily dose (cDDD)] reduced risk of developing HCC [odds ratios (ORs)=0.53,0.36,0.32,and 0.26 in ≤ 60,60–180,181–365,and>365 cDDD,respectively;<0.0001].The study also suggested that risk reduction was apparent in the presence of liver diseases such as chronic viral hepatitis,liver cirrhosis,alcoholic liver disease,and previous cancer (OR=0.27,95%CI:0.14–0.50),but not significant in cases without liver disease (OR=0.64,95%CI:0.32–1.29).Similar reports from Taiwan showed a doseresponse relationship between statin use and the risk of HCV and HBV in an HCV cohort (HR=0.66,0.41,and 0.34 in 28–90,91–365,and>365 cDDD,respectively;<0.0001) and in an HBV cohort (HR=0.66,0.47,and 0.33 in 28–89,90–180,and>180 cDDD,respectively;<0.0001)[46,47].In a cohort of 7248 HCV-infected patients in the United States ERCHIVES database,statin use was linked with a 44% decrease in the development of cirrhosis and a 49% decrease in incident HCC.Atorvastatin and fluvastatin were associated with more significant antifibrotic effects than other statins[48],and in 18080 patients with nonalcoholic fatty liver disease without cirrhosis,even higher HCC suppressive effects were suggested (HR=0.29)[49].Several reports have indicated that statins prevent liver fibrosis,and statins may delay the development of HCC by preventing fibrosis and inflammation of the liver[50].A phase II trial to investigate the efficiency of a simvastatinplacebo on the change in serum AFP-L3%from baseline to 6 mo following treatment initiation in cirrhotic patients with endstage liver disease (NCT02968810) is currently underway.Atorvastatin is being investigated for tertiary prevention after curative resection or ablation for HCC (SHOT trial,NCT03024684).
STATINS AND PANCREATIC CANCER
A population-based case-control study of incident CRC in northern Israel showed that specific polymorphisms in thegene modify the protective association between statins and CRC risk.Compared with non-statin users,the unadjusted OR of CRC among statin users with the A/A genotype of rs12654264 inwas 0.3(95%CI:0.18–0.51) and 0.66 among statin users with the T/T genotype (95%CI:0.41–1.06;=0.0012)[71].
RCTS
Many retrospective cohort studies have identified a reduced risk of cancer mortality in patients taking statins to control cholesterol.However,prospective clinical studies have mostly not been successful (Table 1)[29,30,59-61].Several causes might interpret these differences,including interpatient differences in the type of statins and the dose and duration of statin use.Besides,it is possible that not all cases benefit equally from statin treatment.
By this time Vivien s active impatience had subsided67 into passive weariness, his yawns were continual and scandalous, but nobody heeded69 him, he stared hopelessly at the thick black curtain which hung down straight in front of him, and could hardly believe his eyes when it presently began to slide back, and he saw before him the Black Bird
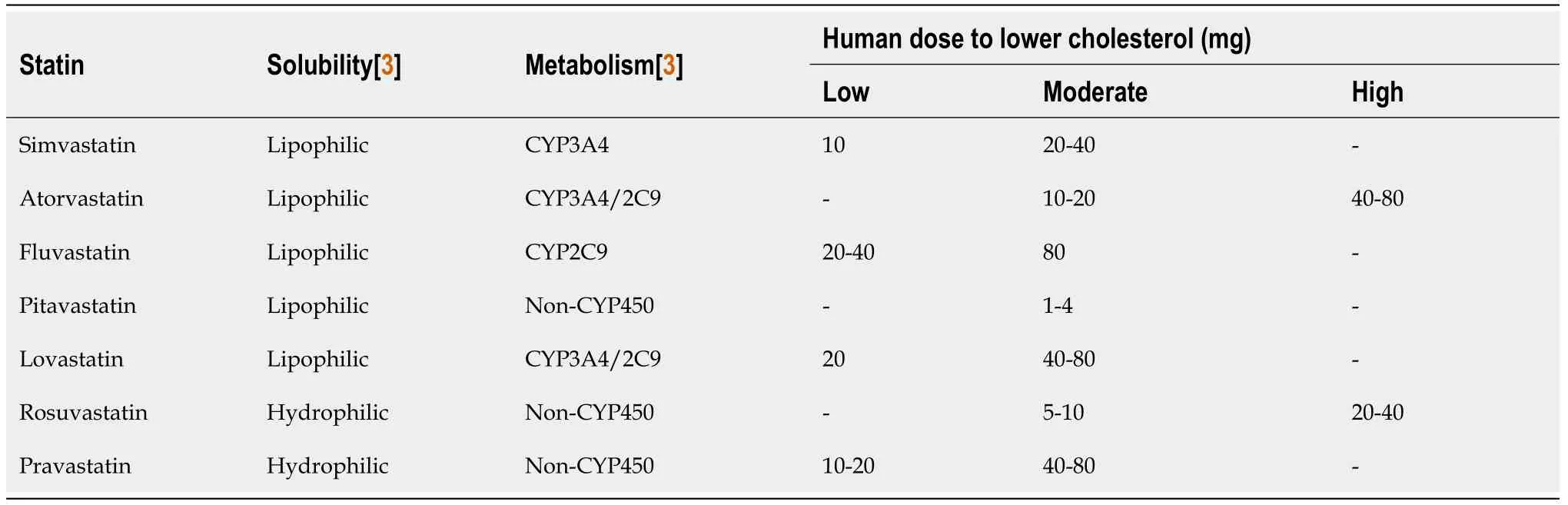
There are seven types of statins (simvastatin,atorvastatin,fluvastatin,lovastatin,pitavastatin,rosuvastatin,and pravastatin) that can be prescribed for hypercholesterolemia worldwide (Table 2).However,which statins are most effective against cancer remains unclear.In manystudies,lipophilic statins are more effective in antiproliferation ability.Because lipophilic statins can cross biological membranes without requiring specific transporters,they have greater intracellular access and are thought to have more effective mechanisms than hydrophilic statins.One report examined differences in the effect of statins on pancreatic cancer usingstudies[62].While simvastatin exerted the highest tumor suppressive effects,rosuvastatin and fluvastatin were the most potent compounds in an animal model.A retrospective cohort study examining the effects of different types of statins on advanced prostate cancer treated with androgen deprivation therapy found that atorvastatin,pravastatin,rosuvastatin,or pitavastatin showed a stronger effect on reduction in mortality compared with other statins[63].It is necessary to determine the type of statin most effective against cancer to plan an optimal RCT.
Then the knight said, It is very strange that the tree should belong to you, and yet that you have not the power to break anything from it! But they would have that the tree was theirs; and while they were saying this, Little Two-eyes rolled a couple of golden apples from under the cask, so that they lay at the knight s feet, for she was angry with Little One-eye and Little Three-eyes for not speaking the truth
Two p53 mutants with gain-of-function mutations were shown to interact with nuclear SREBP2 and enhance the gene transcription of MVA pathway[12].In contrast,wild-type p53 reduces lipid production by increasing LPIN1 expression under conditions of glucose starvation[13].The tumor suppressor protein RB has also been involved as a MVA pathway regulator by interacting with SREBPs and reducing their binding to promoters of target genes[14,15].The oncoproteins Yes-associated protein(YAP) and transcriptional co-activator with PDZ-binding motif (TAZ),both mediators of the Hippo pathway,are controlled by the SREBPs/MVA pathway[16].The geranylgeranyl pyrophosphate generated by the MVA cascade is essential for activation of Rho GTPases that,in turn,activate YAP/TAZ by inhibiting their phosphorylation and promoting their nuclear accumulation (Figure 2).
BIOMARKERS TO IDENTIFY CANCERS FOR WHICH STATINS ARE EFFECTIVE
SREBPs
A recent report showed that the MVA pathway is involved in T lymphocyte metabolism and regulates T cell differentiation[20].Improved understanding of MVA metabolism will enhance more efficient T cell manipulation for immunotherapy in cancer treatment.
The coachman perceived that the shepherd wished to follow her, and warned him not to do so if he valued his life; but the shepherd wouldn t listen to his advice
HMGCR
HMGCR is directly inhibited by statins,and SREBPs increaseexpression through a feedback mechanism that is induced when intracellular cholesterol is depleted (Figure 1).High HMGCR protein expression is associated with poor prognosis in various cancers[65-67].The efficacy of statins for cancer is inversely linked with high expression of cholesterol biosynthesis genes,including thegene[64,68].However,other reports suggested that HMGCR expression alone could not accurately predict the effect of statins[65,69].Whether HMGCR expression alone can accurately predict statin susceptibility remains unclear.One possible interpretation for the conflicting data is the poor specificity of many commercially available HMGCR antibodies[70].Further comprehensive studies using validated HMGCR reagents are required to properly investigate the utility of HMGCR expression as a predictive biomarker of the effects of statins.
A meta-analysis of 26 studies showed a considerable reduction in pancreatic cancer risk with statin use [relative risk (RR)=0.84,95%CI:0.73–0.97;<0.001][51].In subgroup analyses of the study,a non-significant relation was found between longterm statin use and the risk of pancreatic cancer (RR=0.98,95%CI:0.86–1.11;=0.718).There was a non-significant relation between the use of lipophilic statins and the risk of pancreatic cancer (RR=0.98,95%CI:0.84–1.15;=0.853).On the other hand,several studies revealed a reduced risk of pancreatic cancer among statin users[52-54],other reports showed no evidence of an association between statin use and pancreatic cancer[52,55].A retrospective study of 2427 pancreatic cancer patients showed a 31% reduction in mortality in the group taking simvastatin and a 39%reduction in the group taking atorvastatin[56,57].In another study of 1761 pancreatic cancer patients,the 5-year OS rate was 16.6% for statin users and 8.9% for nonusers (=0.012)[57].Among 226 patients undergoing resection for pancreatic cancer,active use of moderate-to high-dose simvastatin was linked with favorable OS and disease-free survival[58].
The further the Prince went the more he noticed that the pocket in which the little roll of linen lay became heavier, and in proportion his heart grew lighter18
Mesenchymal cell markers
Several studies have demonstrated that tumor cells with higher vimentin expression(mesenchymal cell marker) and lower E-cadherin expression (epithelial cell marker)are highly sensitive to statin treatment[72-74].Total vimentin and E-cadherin expression are not appropriate markers for the sensitivity of statins,but abundant cytosolic vimentin and absent cell surface E-cadherin expression indicate sensitivity to statins[73].HRAS-induced epithelial-to-mesenchymal transition (EMT) through activation of zinc finger E-box binding homeobox 1 sensitized tumor cells to the antiproliferative activity of statins[74].These studies also showed that statins preferentially kill cells induced to undergo EMT,suggesting that statins may be more effective against metastatic disease and prevent metastasis.
The king often lost his patience, and was determined8 to see his daughter, but the queen always put him off the idea, and so things went on, until the very day before the princess completed her fourteenth year
p53
Wild-type p53 represses the MVA pathway[12],while loss ofand two gain-offunctionmutants have been reported to enhance the expression of MVA pathway genes[11,75].Tumors with loss ofor the two gain-of-function mutations are particularly vulnerable to statin treatment[76-78].
RAS mutations
The FPP and geranylgeranyl pyrophosphate produced by the MVA pathway serve as substrates for the post-translational prenylation of RAS.Therefore,RAS mutations have been hypothesized to be potential biomarkers of statin sensitivity.However,preclinical studies have shown that RAS mutation alone cannot predict statin susceptibility[74,79].In a subgroup analysis of retrospective studies of CRC,statins were shown to have a higher prognostic effect in cancers withmutations[80].However,other studies have reported no association between statin effects on CRC andstatus[39,81].Further studies are needed to evaluate the utility ofmutation status to predict the effect of statins on cancer.
ER
In breast cancer,the effect of statins has been linked with ER status,in which ERnegative breast cancer cells are notably sensitive to statin treatment[67].These preclinical findings are further strengthened by clinical data demonstrating greater tumor cell apoptosis after fluvastatin treatment in women with ER-negative breast cancer[82].
COMBINATION OF STATINS WITH EPIDERMAL GROWTH FACTOR RECEPTOR INHIBITORS
Several clinical trials have examined the introduction of simvastatin to epidermal growth factor receptor (EGFR) inhibitors therapy for-mutated CRC patients.The hypothesis behind these clinical trials is that the statin-induced depletion of MVA will inhibitprenylation,which will inhibit membrane localization and enhance the effectiveness of EGFR inhibitors[83,84].Unfortunately,most trials have failed to show significant survival benefits from statins[85-87].These results may suggest thatmutation status is not a predictive biomarker of response to statin treatment.Another clinical trial showed that the addition of simvastatin to a cetuximab/irinotecan regimen overcame cetuximab resistance[88].In this clinical trial,the therapeutic benefit of statin was only detectable in patients bearing tumors with mutantand a low Ras signature[88].The Ras signature score is derived from the expression of Ras pathway-related genes across multiple databases and reflects other possible aberrations such asandmutations.Hence,factors other thanmutation must be considered to predict the efficiency of statins in overcoming resistance to anti-EGFR therapy.
COMBINATION OF STATINS WITH RADIATION THERAPY
Statins may have synergistic effects with radiation therapy (RT) on cancer and may reduce inflammation and the gut and skin toxicities induced by RT.In retrospective cohort studies,patients taking statins during RT or chemo-RT for rectal,bladder,or prostate cancer treatment showed considerably higher rates of pathological complete response,local control and progression-free survival[89-93].However,no study has shown an apparent benefit[94].Furthermore,statins significantly reduced RT-induced bowel toxicity and skin injury[95-97].However,a single-arm phase II trial of 53 prostate cancer patients taking lovastatin showed no reduced incidence of grade 2 or higher rectal toxicity compared with historical controls[98].A RCT of simvastatin combined with standard chemotherapy and radiation in preoperative treatment for rectal cancer is underway.
COMBINATION OF STATINS WITH IMMUNOTHERAPY
Mevalonic acid metabolism is involved in controlling T cell activation[19,20,99,100].Statins inhibit the geranylgeranylation of small GTPases,resulting in arrested endosomal maturation,prolonged antigen retention,enhanced antigen presentation,and T cell activation.It has been reported in multiple mouse cancer models that MVA pathway inhibitors are vigorous for cancer vaccinations and synergize with anti-PD-1 antibodies[101].The tumor microenvironment is enriched with cholesterol.The high cholesterol in the tumor microenvironment induces CD8+ T cell exhaustion and upregulates the immune checkpoints PD-1,2B4,TIM-3,and LAG-3[102].Furthermore,lowering cholesterol levels in the tumor microenvironment by simvastatin restores the antitumor activity of CD8+ T cells.Many preclinical studies have demonstrated that the MVA pathway is involved in immune regulation.Future research into the immunomodulatory properties of statins has important clinical implications for cancer immunotherapy.
CONCLUSION
Clinical data that evaluated the utility of statins as anticancer agents have shown responses in some but not all cancers.Optimizing the type,dose,and duration of statins,as well as detecting biomarkers to recognize responders and developing combination therapies,will heighten the value of statins in cancer treatment.
 World Journal of Gastrointestinal Oncology2022年1期
World Journal of Gastrointestinal Oncology2022年1期
- World Journal of Gastrointestinal Oncology的其它文章
- Comment on “Outcomes of curative liver resection for hepatocellular carcinoma in patients with cirrhosis”
- Liquid biopsy:Precise diagnosis and therapy for cholangiocarcinoma
- Increased risk of colorectal neoplasia in inflammatory bowel disease patients with post-inflammatory polyps:A systematic review and meta-analysis
- Exosomes as potential diagnosis and treatment for liver cancer
- Effects of cognitive behavior therapy combined with Baduanjin in patients with colorectal cancer
- Intertwined leukocyte balances in tumours and peripheral blood as robust predictors of right and left colorectal cancer survival