
Application of ablative therapy for intrahepatic recurrent hepatocellular carcinoma following hepatectomy
2023-03-17 07:45RongCongXiaoHongMaShuangWangBingFengWeiCaiZhaoWeiChenXinMingZhao
Rong Cong,Xiao-Hong Ma,Shuang Wang,Bing Feng,Wei Cai,Zhao-Wei Chen,Xin-Ming Zhao
Rong Cong,Xiao-Hong Ma,Shuang Wang,Bing Feng,Wei Cai,Zhao-Wei Chen,Xin-Ming Zhao,Department of Diagnostic Radiology,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China
Abstract The post-hepatectomy recurrence rate of hepatocellular carcinoma(HCC)is persistently high,affecting the prognosis of patients.An effective therapeutic option is crucial for achieving long-term survival in patients with postoperative recurrences.Local ablative therapy has been established as a treatment option for resectable and unresectable HCCs,and it is also a feasible approach for recurrent HCC(RHCC)due to less trauma,shorter operation times,fewer complications,and faster recovery.This review focused on ablation techniques,description of potential candidates,and therapeutic and prognostic implications of ablation for guiding its application in treating intrahepatic RHCC.
Key Words:Hepatocellular carcinoma;Recurrence;Ablation techniques;Radiofrequency ablation;Combined therapy;Therapeutic index
lNTRODUCTlON
Hepatocellular carcinoma(HCC),with high morbidity,mortality,and recurrence rates,remains a global health challenge[1].Surgical resection is considered the main strategy for long-term survival of patients with HCC.However,the incidence of recurrence reaches approximately 70% 5 years after hepatectomy,even in patients with a single tumor ≤ 2 cm[2].Advances in preoperative prediction and postoperative follow-up strategies have facilitated the earlier detection of recurrent HCC(RHCC)[3-5],allowing for more treatment options.Thus,an appropriate therapeutic option is crucial for achieving long-term survival of patients with recurrence after surgery,which requires a comprehensive understanding of possible treatments and thorough evaluation of the patient.
With the necessity to fully consider the initial treatment,the clinicopathologic characteristics of primary HCC,recurrence interval,the characteristics of RHCC,general condition of the patient's liver,and other factors[6,7],treating RHCC cannot exactly follow the guidelines for primary HCC.Considering that inadequacy of residual liver volume,postoperative liver decompensation,intraabdominal adhesions and anatomical variation following initial resection increase difficulty and risk of re-resection,only about 19% of well-selected patients can receive secondary surgery for a definite survival benefit in clinical practice[8,9].Ablation as a curative but less invasive treatment may be considered in the management of RHCC.
Local ablative therapy has been established as a treatment option for resectable and unresectable HCCs according to current clinical guidelines[3,10],which can provide a sustained complete response,a lower complication rate,and a 5-year survival rate of 68.5% for early HCC,even initially operable HCC[11].The extensive and promising application of ablation in primary HCC makes it a feasible approach for the treatment of intrahepatic RHCC.This review demonstrated the role of ablation in treating RHCC,focusing on different ablative techniques,descriptions of potential candidates,as well,therapeutic and prognostic implications for guiding its better application.
RADlOFREQUENCY ABLATlON
Radiofrequency ablation(RFA)is the most commonly used modality for treating both primary and recurrent HCC.Meanwhile,RFA has gained an increasing role owing to its efficacy and safety.When the electrode tip is inserted into the selected tissue to generate electric current,RFA induces ionic agitation,local heat,and subsequent coagulation necrosis[12].Some factors,such as centrifugal heat propagation,“heat-sink effect” mediated by blood perfusion,and increased impedance due to tissue charring limit the size of the ablation zone and reduce the efficacy[13].These also have driven continuous device and procedure improvements:Multi-tined expandable electrodes,internally cooled electrodes,multipolar ablation using bipolar electrodes,and simultaneous vessel obstruction[13-15].
Candidates
For intrahepatic recurrent HCC after hepatectomy,the indications for RFA[16-18]are as follows:Within the Milan criteria at recurrence,satisfying a single lesion(≤ 5 cm in diameter)or three or fewer lesions(each ≤ 3 cm in diameter)without macrovascular invasion or distant metastasis;Child-Pugh grade A or B liver function;Eastern Cooperative Oncology Group performance score of 0 to 1;no uncorrectable coagulation status;no severe varices and intractable ascites;and an acceptable and safe path evaluated by imaging.
Therapeutic and prognostic implications
Baiet al[18]analyzed the long-term survival of solitary RHCC of 5 cm or less after RFA,and the rates of primary technical success,local tumor progression(LTP),and 1-,3-,5-,and 10-year overall survival(OS)post ablation were 94.8%,11.2%,94.0%,71.8%,54.5%,and 33.7%,respectively,in the RHCC following hepatectomy subgroup,which was similar to primary HCC of 5 cm or less after RFA.The safety and efficacy of RFA for RHCC are being gradually affirmed by clinical studies,and an increasing number of retrospective studies comparing repeat hepatectomy and RFA,especially for early stage RHCC,have been reported in recent years.The comparison outcomes of survival between the two groups are conflicting,with inherent selection biases,either equivocal or favorable for one.The majority reported that RFA provided similar OS to repeat hepatectomy for RHCC,with 5-year OS rates of 26%-71%,but with fewer major complications(0%-1.6%vs2.6%-9.1%)and shorter hospital stays(3-5 dvs8-14 d)[19-25].
Xiaet al[17]conducted a randomized clinical trial for comparing long-term survival results following repeat hepatectomy with those following percutaneous RFA in 240 patients with early stage RHCC.They found no significant difference in the 1-,3-,and 5-year OS rates between the two groups(92.5%,65.8%,and 43.6%vs87.5%,52.5%,and 38.5%,respectively).However,RFA was linked to a greater risk of local repeat recurrence and early repeat recurrence than repeat hepatectomy,consistent with the findings of a retrospective multicenter study[25]which concluded that repeat hepatectomy for RHCC within the Milan criteria resulted in longer recurrence-free survival and less frequent early repeat recurrence(less than 12 mo).The rate of inaccurate ablation and the possibility of the presence of satellite nodules increase as the target size of RFA increases in general,leading to an inferior to repeat hepatectomy for local tumor control and a tendency toward a shorter recurrence-free survival of RFA.
A number of factors reported previously were associated with worse survival of RHCC following treatment,including larger and multiple resected tumors,the presence of microvascular invasion(MVI)at initial hepatectomy stage,time to recurrence(TTR)≤ 1 year,poor Child-Pugh class,portal hypertension,serum-fetoprotein(AFP)level greater than 200 ng/mL,larger and multiple RHCC at recurrent stage,etc[18,21-26].These factors resulted in a higher tumor burden,poorer liver function,and more aggressive behavior,which needed to be considered for appropriate therapeutic strategies.
Xiaet al[17]found that percutaneous RFA ablation was related to worse local tumor control and OS than repeat hepatectomy in patients with target diameter > 3 cm or AFP level > 200 ng/mL.Small ablated tumors(≤ 3 cm)can achieve higher complete response rates of > 95%[16,26,27].For larger tumors(> 3 cm),an overlapping ablation strategy,other ablation modalities,or combination of transarterial chemoembolization(TACE)and RFA were required to produce ablation zones more reliably and sufficiently[28].
A previous study[29]focused on RHCC with MVI-positivity at initial hepatectomy and concluded that repeat surgery/RFA can provide a better survival outcome for selected BCLC stage 0-A patients than TACE,which was contrary to the results of Meniconiet al[6]and Jinet al[30]They concluded that TACE seemed more appropriate than curative treatments in a small sample of early stage MVI-positive HCC.Early recurrence(TTR ≤ 1 or 2 years)is generally related to intrahepatic metastases,MVI,and microsatellite lesions generated by primary HCC,with poor survival after hepatectomy[31].Yanget al[32]reported that patients with late recurrence(> 1 year)had better survival outcomes after RFA than those with early recurrence(≤ 1 year).The comparison between repeat hepatectomy and RFA for RHCC with different TTR was conducted in a limited number of studies.Lianget al[19]and Xiaet al[17]found that the OS was similar between the two treatments in patients with a TTR ≤ 1 year or > 1 year.Luet al[33]showed that the post-recurrence survival rates for the repeat hepatectomy group were better than those for the RFA group of patients with early recurrence(TTR ≤ 2 years).However,no significant difference was found in the late recurrence group(TTR > 2 years).Sequential TACE and RFA were found to offer a better OS for patients with recurrence ≤ 1 year than RFA alone,but not for those with recurrence for more than 1 year[28].With the different results of limited studies,treatments for these particular populations will be required further investigation.
Complications
The morbidity and mortality of RFA are obviously lower than those observed following repeat hepatectomy for RHCC,while the rate of complications increases when performing more aggressive procedures for larger tumors and targets at-risk location or at poor liver and general condition.Pain and fever post-ablation are common but remain short after symptomatic treatment.The major complications of RFA include pneumonia,pneumothorax,pleural effusion,hemoperitoneum,ascites,liver hematoma,liver abscess,subdiaphragmatic abscess,liver failure,injury or perforation of adjacent structures such as diaphragm,gallbladder,colon or stomach,ileus,wound or puncture site infection and tumor seeding[17,18,25].A reasonable RFA protocol for well-selected patients is crucial for protecting surrounding tissues and preventing complications.
OTHER AVAlLABLE ABLATlVE TECHNlQUES
Microwave ablation
Microwave ablation(MWA),an emerging alternative modality to RFA,causes thermal coagulation by utilizing microwaves at a frequency of 2450 MHz to induce the vibration and rotation of water molecules within the tissue and subsequent heat generation[34].MWA have theoretical advantages over RFA including a higher temperature,a faster heating of a larger target,a less “heat-sink effect” and insensitivity to tissue conductance[13].The first-generation MWA was initially limited by technical problems related to sub-optimal power handling,large antenna diameter and antenna shaft heating.Its resulting ablation zone is small and more elliptic[35,36].Thus new-generation MWA have developed and simultaneous power delivery technique of multiple antennas has been tried for producing reliable and large spherical ablation zone[37,38].Zhanget al[39]evaluated the efficacy of US-guided percutaneous MWA for RHCC measuring ≤ 5 cm and get 5- and 7-year OS rates of 39.6% and 17.3%,respectively.Ryuet al[40]performed MWA during open surgery in 75 patients with intrahepatic recurrence after hepatectomy and identified MWA as a safe and feasible procedure,which provided a 5-year survival rate of 55.4%,comparable to results reported previously for re-resection,RFA,and MWA for primary HCC.The application of MWA in RHCC was slowly being recognized,and more data will be needed to demonstrate its value for larger RHCC and its efficacy over RFA.
Percutaneous ethanol injection
Ethanol injected into the tissue induces coagulation necrosis mainly because of its dehydronative and protein degenerative effects and partly because of its thromboembolic effect[41].Percutaneous ethanol injection(PEI)could be precisely applied to ablate HCC ≤ 2 cm in diameter,but the necrosis rate is reduced and the local recurrence rate increases for larger tumors[42].Compared to thermal ablation,it is inexpensive and has a low rate of adverse effects even for patients with Child-Pugh class C or tumors at risk locations;however,repeated injections are often required for effective treatment.These characteristics have promoted its application in combination therapies[43].Yinet al[27]treated 288 patients with post-hepatectomy RHCC(maximum diameter ≤ 7 cm and number ≤ 5)using PEI,RFA,MWA,or PEI combined with RFA.The incidence of LTP in the PEI group was 19.5% and no significant difference was found among the four ablative modalities.However,selection bias existed,and the authors did not focus on comparing the efficiencies of the different techniques.
High-intensity focused ultrasound ablation
High-intensity focused ultrasound ablation(HIFU)ablation is an extracorporeal conformal therapy that can achieve heat-induced coagulation necrosis without the need for surgical exposure or probe insertion.Heat generation is mediated by focusing high-intensity ultrasound beams on the target using the extracorporeal motion of a multi-element ultrasound transducer.HIFU,which is noninvasive and conformal,can ablate a large volume of tumor with no worry of tumor seeding along the needle tract[44].The value of HIFU or HIFU combined with TACE in unresectable HCC has been previously reported[44,45].A study[46]showed that HIFU was a safe and feasible treatment modality for RHCC with an acceptably low morbidity rate and a comparable survival outcome to RFA,which was conducted among a small number of patients meeting the Milan criteria.HIFU have not get widespread adoption yet,probably as ultrasound propagation influenced by different tissues,ultrasound artifacts and respiration motion add time consumption and technical challenge relative to other ablation modalities[47].There is no additional clinical data with HIFU for RHCC currently.
Cryoablation
Cryoablation(CRA)is a thermal technique that uses cryoprobes to transfer low temperatures caused by the Joule-Thomson effect with super-cooled gas or liquid expansion,and achieves tissue necrosis by alternating cycles of freezing and thawing,which induces denaturation of cellular proteins,cell membrane rupture,cell dehydration,and ischemic hypoxia[48].Cryoshock,a severe adverse event associated with multiorgan failure post-CRA,has been reported in previous studies,but the new generation of cryoablation systems with ultrathin cryoprobes that use argon-helium may lead to a low risk of bleeding and cryoshock[49].The main advantage of CRA over heat-based ablation modalities is a well-visualized ice ball on ultrasound(US),computed tomography(CT),or magnetic resonance imaging(MRI)during ablation for precise monitoring,which contributes to the potential value of cryoablation for targets larger or close to important structures[48].A multicenter randomized controlled trial showed a significantly lower LTP after CRA than after RFA for HCCs sized 3.1-4.0 cm[50].For RHCC,Chenet al[51]used percutaneous CRA to treat 76 tumors(≤ 7 cm)in 26 recurrent patients and confirmed its efficacy with 1- and 3-year OS rates of 70.2% and 28.8%,respectively;however,further research is insufficient.
Irreversible electroporation
Irreversible electroporation(IRE)works by short pulses of high intensity delivered between two electrodes(convergent centripetal technique),which produce irreversible pores in the cellular bilayer membrane for cell death,while the connective tissue,blood vessels,and bile ducts are preserved.It is a nonthermal ablative method with no influence of the “heat-sink effect”,a lower risk of thermal injury,and less frequent liver failure[13].Therefore,it can be considered for the treatment of dangerous sites and poor liver function[52].This procedure can only be performed in patients with normal cardiac rhythm,because high-intensity pulses can cause myoclonia and severe arrhythmias.Overall,IRE could be indicated for a wider range of candidates than thermal techniques with consideration of patient condition,cost,and operational complexity,although more clinical data are required to validate its efficacy.
Various ablation modalities have their advantages and limitations(Table 1).RFA has been confirmed to be effective and used for RHCC with an increasing frequency;however,available data on other ablation modalities are insufficient,and limited studies have sought to directly compare the effects of various ablation techniques for treating RHCC.
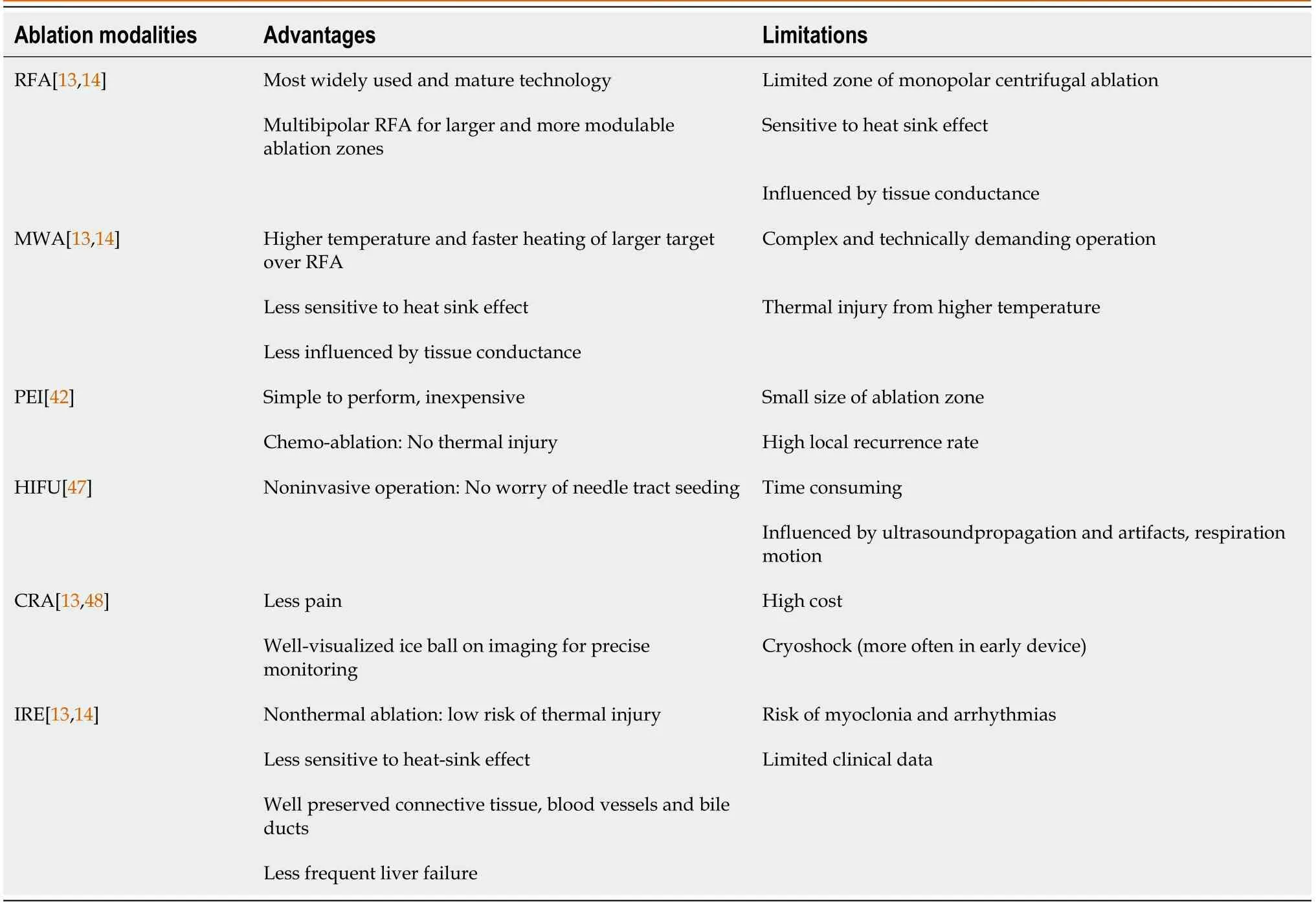
Table 1 Description characteristics of different ablation modalities
ABLATlON lN COMBlNED THERAPY
Various combinations of treatments have been explored to improve the local tumor control and survival outcomes of ablation.The available experience with ablation combination therapy for RHCC has mainly focused on RFA.
RFA and PEI
Ethanol injection can reduce the “heat-sink effect” by destroying vessels within or around the tumors and promoting thermal conduction by lowering the extent of carbonization of the tissue.Therefore,RFA started after PEI completion could induce an enlarged ablation zone with an adequate safety margin compared with RFA alone,improving local control and reducing distant recurrence[53,54].Chenet al[43]retrospectively compared the efficacy and safety of RFA and PEI(RFA-PEI)with repeat hepatectomy in elderly patients(≥ 70 years)with RHCC within the Milan criteria after initial surgery.The 1-,3-,and 5-year OS and RFS rates after RFA-PEI were 78.2%,40.8%,and 36.7%,and 69.5%,37.8%,and 33.1%,respectively,comparable to those of repeat hepatectomy.They confirmed the good efficacy and high safety of RFA-PEI for RHCC,even for patients with poor performance status who urgently require minimally invasive treatments.
RFA and TACE
Because occlusion of blood flow by TACE before RFA reduces the “heat-sink effect” and the hyperthermia of RFA enhances the effect of anticancer agents on cancer cells,the sequential combination of TACE and RFA can extend the ablation zone and promote the ability of TACE to completely destroy the whole lesion.Penget al[55]reported TACE-RFA provides comparable OS and disease-free survival(DFS)to repeat hepatectomy,fewer major complications and shorter hospital stay.Yanget al[56]demonstrated that the 5-year survival of patients with RHCC after hepatectomy was significantly higher in the combination group than in the TACE or RFA group,but there was no significant difference in survival among these three groups with < 3 cm RHCC,consistent with the conclusion of a prospective randomized trial[28].They further confirmed the benefit of the sequential combination treatment for RHCC measuring 3.1-5.0 cm but not for those with tumors 3 cm or smaller and also recommended it for patients with tumors that recurred 1 year or less,which can be explained by the increased chance of clearance of micrometastases in combination treatment.
RFA and systemic treatment
The combination with systemic therapy has been considered effective to impede rapid progression of residual tumors due to inadequate RFA and control advanced HCC[57].Penget al[58]investigated the role of Sorafenib combined with TACE-RFA in the treatment of advanced RHCC after initial hepatectomy and proved its safety,efficacy and superior survival outcomes over sorafenib alone.These benefits might be due to Sorafenib suppressing angiogenesis induced by TACE or inadequate RFA.The combination of RFA and immunotherapy is also considered rationale.Ablation boosts the T cell immune response to improve the efficacy of immunotherapy and immune checkpoint inhibitors block immune escape to reduce recurrence after ablation[59].A retrospective study[60]reported that patients with RHCC had significantly better RFS and OS outcomes in the RFA plus anti-PD-1 group than in the RFA alone group.However,additional trials are required to confirm these interesting findings.
TECHNlCAL lMPROVEMENTS FOR EXTENDlNG THE APPLlCATlON OF ABLATlON
Ablation procedures can be performed percutaneously,laparoscopically,or at open surgery,using various imaging guidance techniques,including US,CT,or MRI.In general,ablation is appropriate for treating lesions within the Milan criteria and distant from the adjacent organs.In addition to the abovementioned ablation modalities and combination treatments,multiple options of performing paths,guidance strategies,and other technical advances may allow extensive access to curative ablation therapy,especially for patients with a poor profile and tumors with large size,invisibility on US,or risk location.
Laparoscopy and laparotomy over percutaneous RFA provide greater exposure and more direct observation of the tumor and surrounding structures and can be used to temporarily occlude blood flow to increase the ablation zone.Santambrogioet al[61]performed laparoscopic thermal ablation for the treatment of intrahepatic RHCCs(within Milan criteria)that required repeated punctures or adjacent to visceral structures.Laparoscopic ablation was proposed as a safe and effective treatment for RHCC,leading to survival and DFS rates similar to those of primary HCC patients undergoing laparoscopic ablation without increasing morbidity.Contrast-enhanced US,CT,MRI,and image fusion can better delineate the target and final extent of the ablation zone,remedying the limitation of lesion invisibility in conventional US.Songet al[62]and Zhaoet al[63]performed US-CT/MRI fusion-guided RFA for recurrent HCC that was subcentimeter or invisible on US,and both achieved technical success and efficacy rates of over 94%.Linet al[64]conducted MWA guided by enhanced liver-specific MRI in 18 patients with small RHCC and achieved 100% technical success rate.
Furthermore,the creation of artificial ascites or artificial pleural effusion,balloon catheter interposition,three-dimensional visualization technology,fluoroscopic real-time guidance,and other assistive techniques are all effective in ablation safety,a high rate of success,and expansion of indications for ablation[65-68].
CONCLUSlON
The role of ablation in intrahepatic RHCC was shown in Figure 1.Unlike primary HCC,RHCCs are usually detected in the early stage but are not amenable to repeat hepatectomy with consideration of inadequate liver remnants,limited liver function reserves,and technical difficulties due to adhesions following initial surgery.The value of ablation as a minimally invasive but curative method is an increasing concern.For patients who are eligible for ablation and repeat hepatectomy,clinicians need to balance the worse local control and lower major complication rates or shorter hospital stays when making ablation decisions.Various ablation modalities and procedures are continuously improving,and combination strategies may add additional benefits,which promote the extended application of ablative therapy.Further exploration of a particular population with risk prognostic factors and sufficient experience on the efficacy of different ablation modalities and techniques in treating RHCC are required and based on randomized clinical trials with larger sample sizes.Moreover,evidence that ablation could boost the immune response raises expectations for its combination with immunotherapy for advanced RHCC.
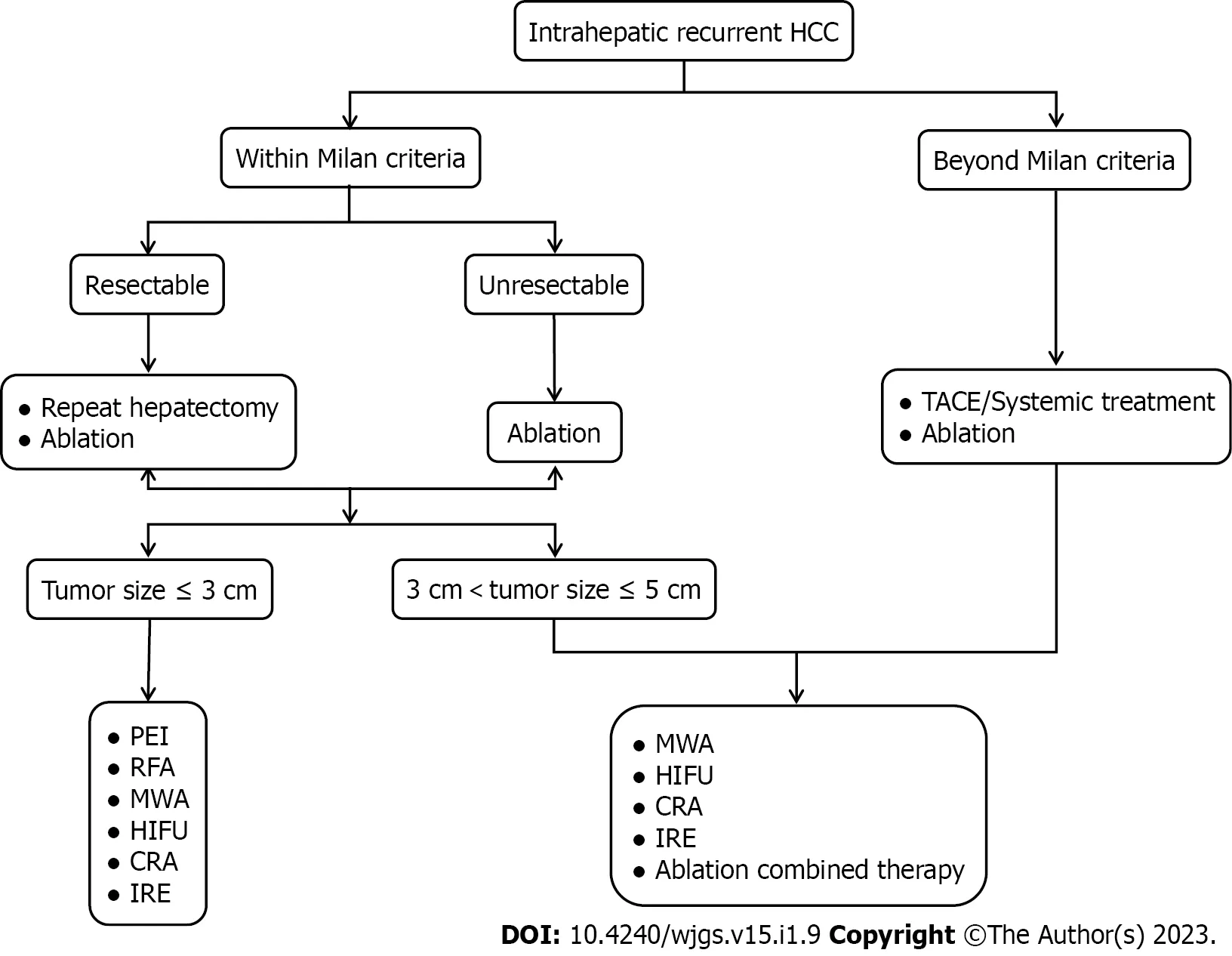
Figure 1 Role of ablation in intrahepatic recurrent hepatocellular carcinoma.HCC:Hepatocellular carcinoma;TACE:Transarterial chemoembolization;RFA:Radiofrequency ablation;MWA:Microwave ablation;PEI:Percutaneous ethanol injection;HIFU:High-intensity focused ultrasound ablation;CRA:Cryoablation;IRE:Irreversible electroporation.
FOOTNOTES
Author contributions:Cong R performed literature review and drafted the manuscript;Cai W and Chen ZW contributed to data collection of the study;Wang S,Feng B,and Zhao XM reviewed the manuscript;Ma XH contributed to conception and design of the study,and critically revised this manuscript;all authors have read and approved the final manuscript.
Supported bythe National Key Research and Development Program of China,No.2020AAA0109503.
Conflict-of-interest statement:The authors declare no conflict of interests for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Rong Cong 0000-0001-9798-6571;Xiao-Hong Ma 0000-0002-9048-8374;Shuang Wang 0000-0001-9241-2018;Bing Feng 0000-0003-1080-9551;Wei Cai 0000-0002-6273-3678;Zhao-Wei Chen 0000-0002-2839-4107;Xin-Ming Zhao 0000-0001-7286-771X.
S-Editor:Chen YL
L-Editor:A
P-Editor:Chen YL
 World Journal of Gastrointestinal Surgery2023年1期
World Journal of Gastrointestinal Surgery2023年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Hereditary polyposis syndromes remain a challenging disease entity:Old dilemmas and new insights
- Postoperative adjuvant therapy for hepatocellular carcinoma with microvascular invasion
- Prognostic effect of excessive chemotherapy cycles for stage ll and lll gastric cancer patients after D2 + gastrectomy
- Development and validation of a novel nomogram for predicting overall survival in gastric cancer based on inflammatory markers
- New perspectives on robotic pancreaticoduodenectomy:An analysis of the National Cancer Database
- lmpact of body mass index in elderly patients treated with laparoscopic liver resection for hepatocellular carcinoma