
Prognostic effect of excessive chemotherapy cycles for stage ll and lll gastric cancer patients after D2 + gastrectomy
2023-03-17 07:45YiFanLiWenBingZhangYuYeGao
Yi-Fan Li,Wen-Bing Zhang,Yu-Ye Gao
Yi-Fan Li,Department of General Surgery,Shanxi Province Cancer Hospital,Taiyuan 030013,Shanxi Province,China
Wen-Bing Zhang,Endoscopy Center,Shanxi Province Cancer Hospital,Taiyuan 030013,Shanxi Province,China
Yu-Ye Gao,Department of Gastrointestinal Surgery,Peking University Cancer Hospital and Institute,Beijing 00010,China
Abstract BACKGROUND According to relevant investigation and analysis,there are few research studies on the effect of excessive chemotherapy cycles after D2 gastrectomy on the survival of patients with gastric cancer.AIMTo determine whether excessive chemotherapy cycles provide extra survival benefits,reduce recurrence rate,and improve survival rate in patients with stage II or III gastric cancer.METHODS We analyzed and summarized 412 patients with stage II gastric cancer and 902 patients with stage III gastric cancer who received D2 gastrectomy plus adjuvant chemotherapy or neoadjuvant chemotherapy.Analysis and comparison at a ratio of 1:1 is aimed at reducing realistic baseline differences(n = 97 in each group of stage II,n= 242 in each group of stage III).Progression-free survival,overall survival and recurrence were the main outcome indicators.RESULTS When the propensity score was matched,the baseline features of stage II and III gastric cancer patients were similar between the two groups.After a series of investigations,Kaplan-Meier found that the progression-free survival and overall survival of stage II and III gastric cancer patients were consistent between the two groups.The local metastasis rate(P = 0.002),total recurrence rate(P < 0.001)and distant metastasis rate(P = 0.001)in the ≥ 9 cycle group of stage III gastric cancer were statistically lower than those in the < 9 cycle group.The interaction analysis by Cox proportional hazard regression model showed that intestinal type,proximal gastrectomy,and ≥ 6 cm maximum diameter of tumor had a higher risk of total mortality in the < 9 cycles group.CONCLUSION Overall,≥ 9 chemotherapy cycles is not recommended for patients with stage II and stage III gastric cancer because it has an insignificant role in the prognosis of gastric cancer.However,for patients with stage III gastric cancer,≥ 9 cycles of chemotherapy was shown to significantly decrease recurrence.
Key Words:Gastric cancer;Propensity score matching;Chemotherapy cycles;Overall survival;Progressionfree survival;Recurrence
lNTRODUCTlON
Common cancer cases in the world include gastric cancer which is also the main cause of human cancer death[1].Specifically,gastric cancer,one of the most common cancers in the world,has a survival rate of only 20%.Stomach cancer is a malignant tumor in which cancer cells attach to the gastric mucosa and gradually spread throughout the body.At the beginning,there are no special symptoms of gastric cancer and the patient is unaware of the problem.However,with the extension of time and the deterioration of the disease,patient's stomachs are gradually unable to digest,causing discomfort.In the final stages,gastric cancer patients will vomit,experience pain,and in severe cases will cough up blood.They present with abdominal swelling,lymph node metastasis and so on.According to the relevant data,the production of gastric cancer is affected by different factors.The initial symptom may be chronic gastritis or bacterial infection,or the gastrointestinal discomfort caused by genes and adverse environment,which may turn into gastric cancer.Among them,the most important factor affecting the occurrence of gastric cancer is the bad environment.If the soil or water contains excessive nitrate and other chemical elements,it is very likely to lead to the occurrence of gastric cancer,and people will inevitably ingest these elements during the diet.In daily life,salty food can also lead to stomach cancer.Moldy food can also cause stomach cancer if consumed for a long time.Generally speaking,the incidence of gastric cancer in women is much lower than that in men,and the most important type of gastric cancer is adenocarcinoma,including diffuse gastric cancer and intestinal gastric cancer.The older people are,the more likely they are to develop stomach cancer,ranging in age from 50 to 80.The incidence of stomach cancer of our people is not low in the global scope,and is far higher than the world average level.Stomach cancer accounts for nearly a quarter of cancer deaths.In the early stages of gastric cancer,when there is no lymphatic metastasis,endoscopic treatment is recommended.In the middle stage of gastric cancer,when the cancer cells are not yet spreading throughout the body,it can be treated by D2 gastrectomy.After the tumor is removed,adjuvant therapy is given postoperatively to reduce the likelihood of bacterial infection and avoid the risk of death.
Although D2 gastrectomy and postoperative adjuvant therapy are the only radical methods for the treatment of gastric cancer at this stage,patients with stage Ⅱ and Ⅲ gastric cancer have a higher recurrence rate after surgery and do not have a higher long-term survival rate.In academia,experts and scholars have discussed the value and effect of postoperative adjuvant chemotherapy for gastric cancer.With the development of the times and the progress of society,more and more people analyze the influence of postoperative adjuvant therapy on gastric cancer patients through experiments and research contents.In this context,people increasingly affirm the value of postoperative adjuvant chemotherapy for gastric cancer.According to relevant data,postoperative adjuvant chemotherapy reduced the mortality rate by more than 20% compared with surgery alone.Therefore,the comprehensive treatment mode of surgery combined with adjuvant chemotherapy has been used more frequently in the treatment of gastric cancer.However,at present,the duration of adjuvant therapy after radical gastrectomy has not been determined,and the correlation between the length of chemotherapy cycles and the effect of chemotherapy is not clear.In other words,with the development of the times,D2 gastrectomy[2]and subsequent adjuvant chemotherapy are constantly improved,and the overall survival period(OS)of gastric cancer patients has been well transformed,but from the perspective of long-term survival,there are still limitations[3,4].
Excessive chemotherapy cycles to treat gastric cancer has been proposed,but the survival benefit has not been determined.According to the Chinese Society of Clinical Oncology clinical guidelines[5]for the diagnosis and treatment of gastric cancer,preoperative neoadjuvant chemotherapy is recommended for 2-4 cycles,and perioperative neoadjuvant chemotherapy is recommended for 2-4 cycles before surgery and 6-8 cycles after surgery.Therefore,≥ 9 cycles of chemotherapy would be considered as excessive chemotherapy cycles.
In our previous study[6]of patients with stage II and stage III gastric cancer,the mean of chemotherapy cycles was 9.65 ± 3.86 and 9.87 ± 3.84,respectively.In addition,we analyzed 1-,3- and 5-year survival rates for patients receiving < 9 cycles of chemotherapy,and found them to be 92.4%(257/278),66.9%(186/278),and 46.4%(129/278),respectively.The 1-,3-,and 5-year survival rates for patients receiving ≥ 9 cycles of chemotherapy were found to be 92.5%(577/624),62.9%(393/624),and 46.3%(289/624),respectively.
In essence,chemotherapy can be both good and bad for patients.Excessive chemotherapy cycles(≥ 9)give rise to unpleasant side effects and harmful effects on physical function.However,the appropriate number of chemotherapy cycles may eliminate any residual cancer cells.The ultimate aim of our research was to determine whether excessive chemotherapy cycles(≥ 9)increase survival and decrease recurrence in patients with stage II and III gastric cancer.
MATERlALS AND METHODS
Data collection
We summarized the relevant data from 2002 to 2020 of more than 400 patients with stage II gastric cancer and 900 patients with stage III gastric cancer who underwent gastrectomy for the treatment of gastric cancer.According to the data,lymph node dissection was higher than D2(complete removal of group 1 and group 2 Lymph nodes).The clinicopathological characteristics included age at surgery,sex,nerve invasion,vascular invasion,number of positive lymph nodes,depth of tumor invasion,number of chemotherapy cycles,TNM stage(according to the 8th edition of the American Joint Board on Cancer),maximum tumor diameter,Lauren classification,retinal metastasis,type of gastrectomy,chemotherapy administration,surgical margin,multi-organ resection,chemotherapy protocol,and group Clavien-Dindo grading of texture,multiple metastases,OS,complications,and progression-free survival(PFS).The number of postoperative chemotherapy cycles,the number of neoadjuvant chemotherapy cycles,medical records,surgical records and follow-up data were analyzed retrospectively.
The inclusion criteria consisted of:(1)Neoadjuvant chemotherapy or adjuvant chemotherapy before radical gastrectomy;(2)Histologically proven gastric cancer;(3)There was no serious damage to the organs after the operation;(4)Complete clinicopathological and follow-up data;and(5)Except for gastric cancer,there were no other malignancies or causes of death.Exclusion criteria are classified as follows:(1)There is no complete clinical data;(2)Other systemic tumors;(3)Non gastric cancer was confirmed by pathological classification;and(4)Bypass surgery and palliative surgery.
The American Joint Board on Cancer's 8 TNM grade reclassified tumor stages.Because this study is retrospective,consent is not required.After a series of reviews,the Ethics Committee of Shanxi Cancer Hospital finally approved the study.This study was consistent with the standards of the Declaration of Helsinki,so patient anonymity was adopted and patient data and information were not disclosed to the public.The specific research content and process are shown in Figure 1.
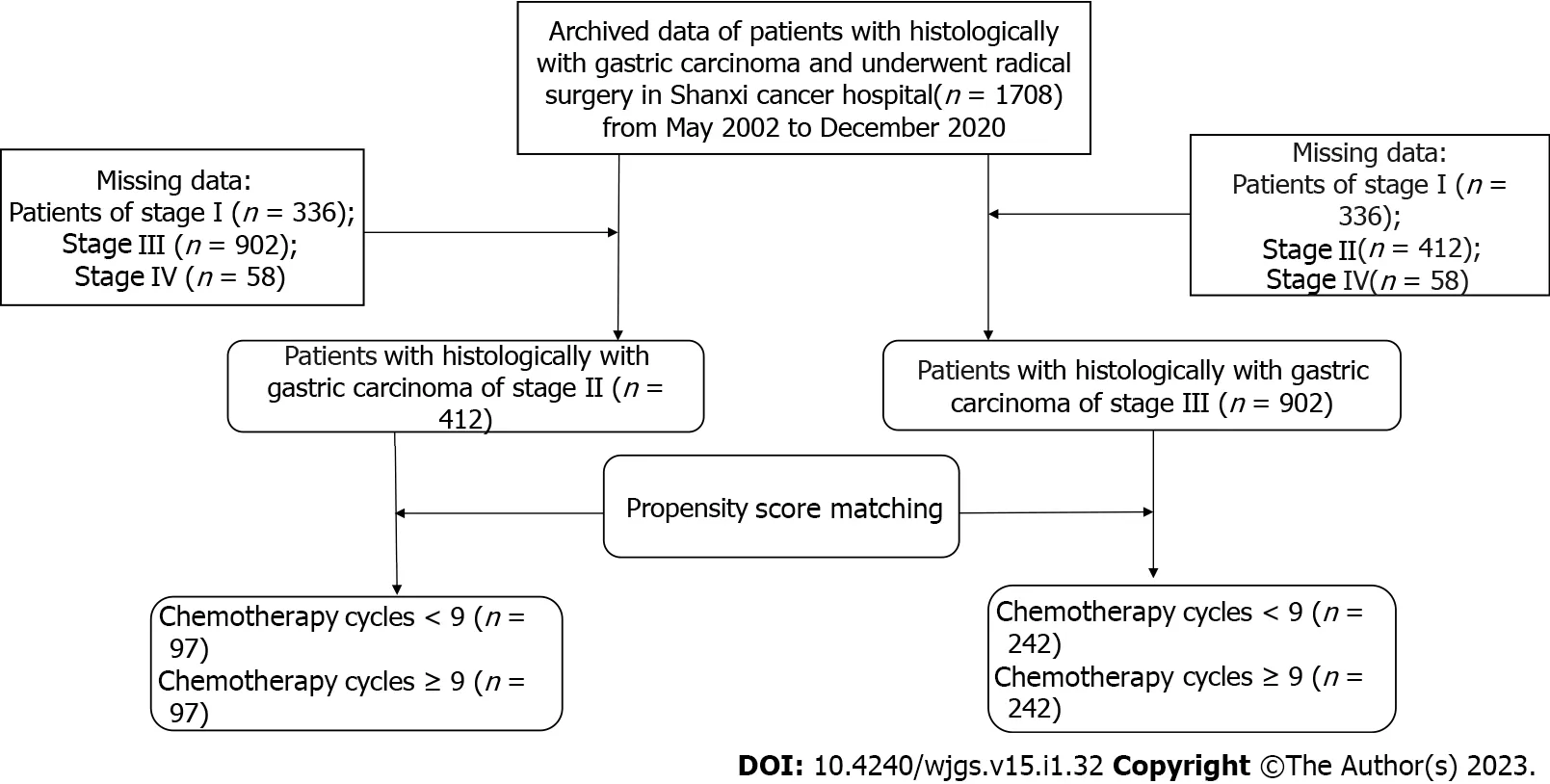
Figure 1 Flowchart of study population enrollment.
Patients received individualized chemotherapy regimens.This paper summarized the dose ranges and other details of several common regimens:(1)Oxaliplatin(130 mg/m2),S-1 and oxaliplatin(SOX),S-1(40-60 mg),the above-mentioned drugs twice a day,the 1stto 14thd,rest for 7 d;(2)S-1,the aforementioned drug twice daily,with the specific dose schedule determined by the patient's area.From day 1 to day 14,40-60 mg,then rest for 7 d;(3)S-1 + apatinib,apatinib(500 mg)administered once daily continuously and S-1(40-60 mg)administered twice daily on day 1 to day 14,then rest for 7 d;(4)Folinic acid,fluorouracil,and oxaliplatin(FOLFOX),folinic acid(200 mg/m2),fluorouracil(2800 mg/m2),and oxaliplatin(85 mg/m2)administered every 3 wk;(5)Oxaliplatin and capecitabine(also known as XELOX)were given intravenous oxaliplatin(150 mg/m2)on the 1stday of every three cycles and orally capecitabine(1000 mg/m2)twice a day from day 1 to day 14,followed by a rest for 7 d;(6)Capecitabine was taken orally twice a day(1000 mg/m2),with a rest of 7 days from day 1 to day 14;(7)Cisplatin and fluorouracil(also known as DCF),S-1 + docetaxel,cisplatin(75 mg/m2),docetaxel(75 mg/m2)on day 1 to day 5,fluorouracil(750 mg/m2)on day 1 to day 5,S-1(40-60 mg)on day 1 to day 14,orally twice a day,then rest for 7 d;and(8)Oral administration of defluoruridine(1000 mg/m2)twice a day from day 1 to day 28,followed by rest for 14 d.
All excised specimens were examined to determine the histological response to neoadjuvant chemotherapy and pathological staging.The number of surviving tumor cells in the tumor determines the grade of tumor regression.According to Ryan criteria[6]:Grade 0(complete response),no residual tumor cells.Grade 1(primary remission),with scattered tumor cells;Grade 2(moderate remission),tumor cell aggregation with fibrosis;Grade 3(mild remission),with substantial tumor cell retention.The toxicity associated with neoadjuvant chemotherapy was evaluated according to Standard 5.0,a common term for adverse events[7].
Follow-up
Patients were followed up until December 2020.The second-stage follow-up was 41.51 ± 21.18 mo,and the third-stage follow-up was 43.56 ± 24.45 mo.Follow-up was conducted every 3 mo for 1 year after surgery,every 6 mo for 2 years to 5 years,and annually thereafter.Routine follow-up included laboratory tests,physical examinations,pelvic ultrasound,chest radiographs,magnetic resonance imaging,and computed tomography.
Statistical analyses
Sex,age at surgery,vascular invasion,nerve invasion,depth of tumor invasion,number of positive lymph nodes,Lauren classification,maximum tumor diameter,type of gastrectomy,and human epidermal growth factor receptor-2(HER2)status were used for propensity score matching(PSM)using 1:1 nearest neighborhood with no replacement and calipers adjusted for sample size and matching success.If a patient is a match,a correlation analysis of primary and secondary endpoints will be performed.The main contents are PFS and OS.The secondary endpoints were tumor recurrence and metastasis,multiple metastases,and recurrence patterns.
Each group generated a Kaplan-Meier survival curve using a log-rank comparison.The category variable analysis was tested using appropriate tests.ThePvalues on both sides were 0.05,which had statistical value.The date of return visit is calculated from the date of surgery to the time of last contact.OS is the time between surgery and death or the last follow-up.PFS refers to the time between surgery and the first recorded death or recurrence.
All data were analyzed and explored using SPSS v25.0 software(IBM Corp.,Armonk,NY,United States).The classification variable was expressed as percentage,and the test methods used in the analysis were Fisher's exact test and chi-square test.Continuous data were expressed as mean ± standard deviation,andt-test was used for analysis.Survival analysis of PFS and OS was performed using Kaplan-Meier method,which was compared with the log-rank test method.Median was used for the non-normal distribution parameters,and the analysis method was Mann-Whitney test.Subgroup analyses were performed by the Cox hazard regression model.P< 0.05 was considered statistically significant.PSM was performed with the Hansen and Bowers overall balance test.Relative multivariate imbalance L1 test was used to determine standardized mean difference < 0.25.Theχ2test was used to compare the differences in recurrence,local-regional recurrence,peritoneal metastasis,and distant metastasis between the two groups.
Nonetheless,the interaction effect between chemotherapy cycles and Lauren classification,types of gastrectomy,and maximum diameter of the tumor on OS were determined for the first time.
RESULTS
PSM and subgroup analysis of TNM stage II gastric cancer patients
Patients in the < 9 cycles group received the following chemotherapy regimens:(1)1 patient received S-1;(2)28 patients received SOX;(3)4 patients received S-1 + docetaxel;(4)10 patients received deofuridine;(5)3 patients received XELOX;(6)32 patients received FOLFOX;and(7)18 patients received multiple regimen combinations.Patients in the ≥ 9 cycles group received the following chemotherapy regimens:(1)61 patients received S-1;(2)6 patients received SOX;(3)9 patients received S-1 + apatinib;(4)15 patients received capecitabine;(5)2 patients received FOLFOX;and(6)5 patients received multiple regimen combinations.Three patients in the < 9 cycles group and 21 patients in the ≥ 9 cycles group received neoadjuvant chemotherapy plus adjuvant chemotherapy.Ninety-four patients in the < 9 cycles group and 76 patients in the ≥ 9 cycles group received only postoperative adjuvant chemotherapy.
All patients with TNM stage II(n= 412)were grouped based on nine variables(sex,vascular invasion,nerve invasion,number of positive lymph nodes,depth of tumor invasion,maximum tumor diameter,Lauren classification,type of gastrectomy,and HER2 status)according to the cycles of chemotherapy received(< 9 cyclesvs≥ 9 cycles)(Table 1).Significant differences in sex(P= 0.022)and age(P< 0.001)were observed between the < 9 cycles groupvsthe ≥ 9 cycles group before PSM.However,after PSM,in which 194 patients were included(97 patients in the <9 cycles group and 97 patients in ≥ 9 cycles group),no significant differences were observed between the two groups(P> 0.05).The Hansen and Bowers overall balance test indicated that the distribution between the two groups was well balanced after PSM(Figures 2 and 3).
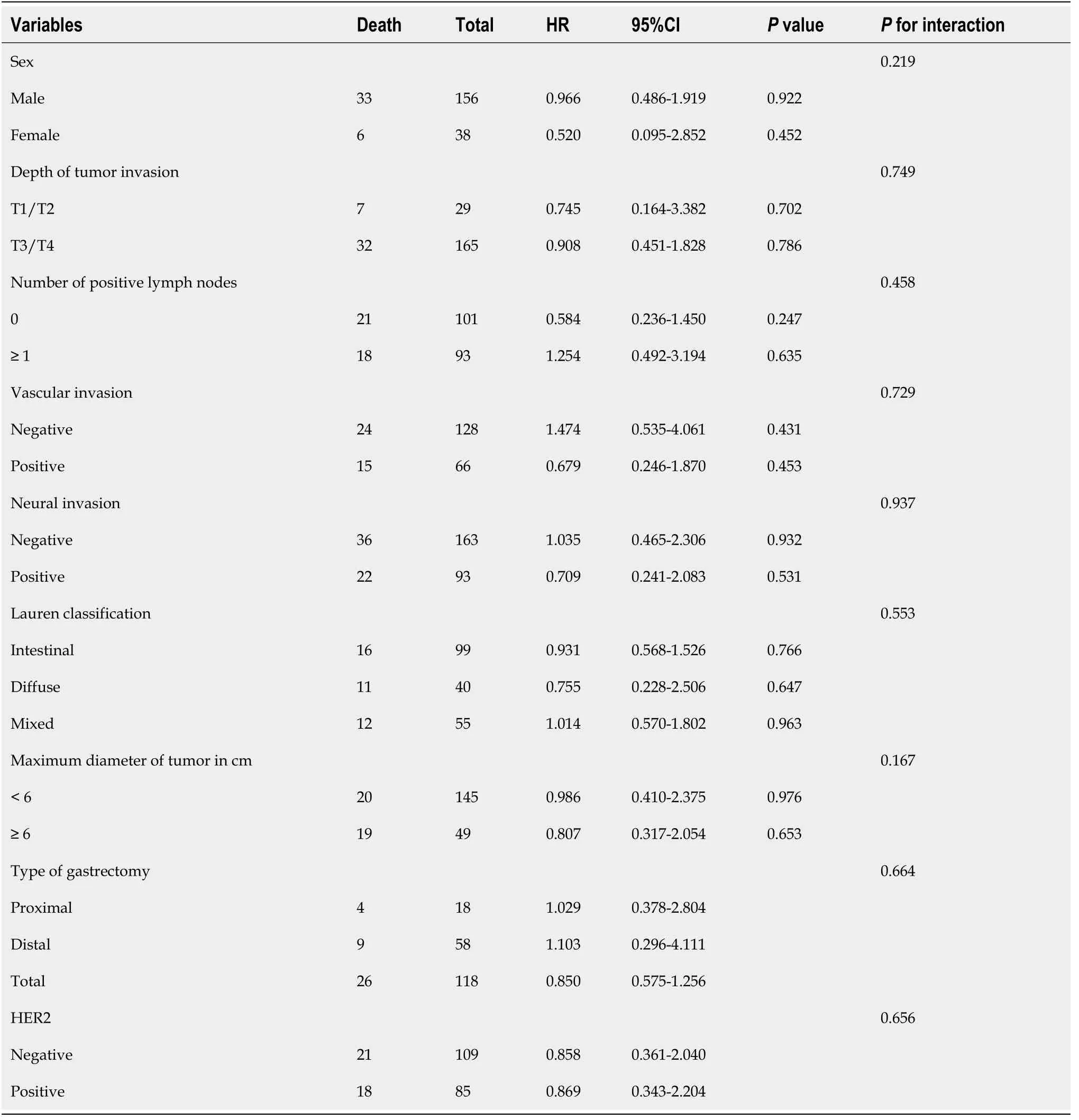
Table 2 Subgroup analysis of overall survival by Cox regression analysis of stage ll gastric cancer patients
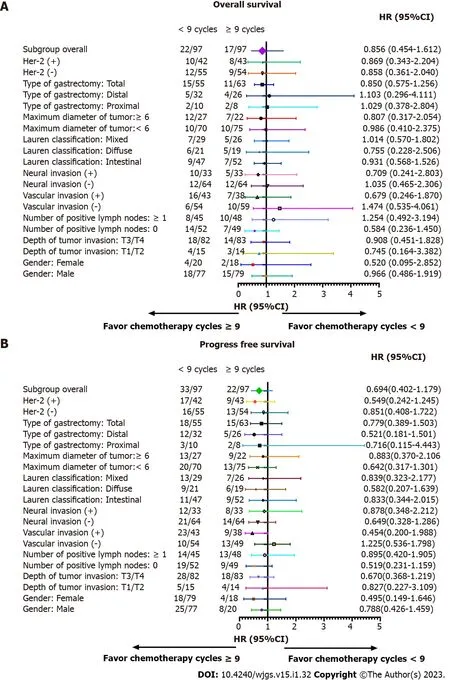
Figure 3 Subgroup analysis of overall survival and progression-free survival based on chemotherapy cycles in stage ll gastric cancer patients.A:Overall survival;B:Progression-free survival.
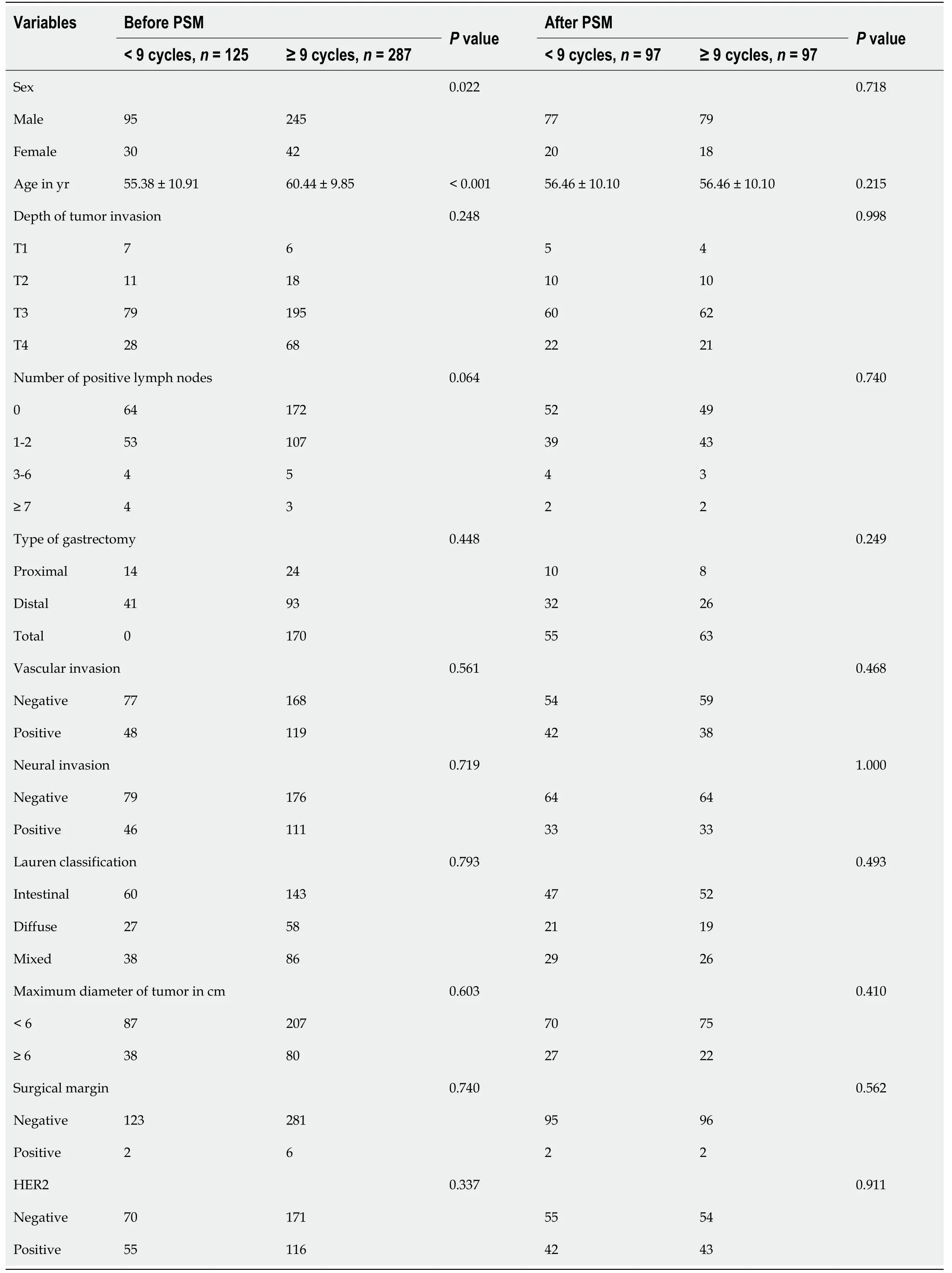
Table 1 Patient characteristics before and after propensity score matching based on the number of chemotherapy cycles for stage ll gastric cancer
OS and PFS were similar in both groups before and after PSM(P> 0.05),indicating that in patients with stage II gastric cancer ≥ 9 chemotherapy cycles does not impart a survival benefit(Figures 2 and 3).In detail,the 1-year OS rate(96.9% vs97.9%,log-rankP= 0.650),3-year OS rate(89.7%vs89.7%,logrankP= 1.000),and 5-year OS rate(79.4%vs83.5%,log-rankP= 0.460)were not statistically different.The 1-year PFS rate was statistically different between the ≥ 9 cycles group and the < 9 cycles group(93.8%vs82.4%,log-rankP= 0.015,respectively).However,that benefit was not observed in the 3-year PFS rate(76.3%vs81.4%,log-rankP= 0.379)and in the 5-year PFS rate(69.1%vs77.3%,log-rankP= 0.195).No differences were observed between the < 9 cycles group and the ≥ 9 cycles group for recurrence(22.7%vs12.4%,respectively,P= 0.059),local-regional metastasis(11.3%vs11.3%,respectively,P= 0.117),and distant metastasis(5.2%vs6.2%,respectively,P= 0.204).
We performed subgroup analyses according to depth of tumor invasion,sex,vascular invasion,number of positive lymph nodes,Lauren classification,neural invasion,types of gastrectomy,maximum diameter of tumor,and HER2 in order to determine if a survival benefit of ≥ 9 cycles was evident in specific patient populations.After subgroup analysis,the differences in OS and PFS between the two groups were not statistically significant(Tables 2 and 3,and Figure 3).
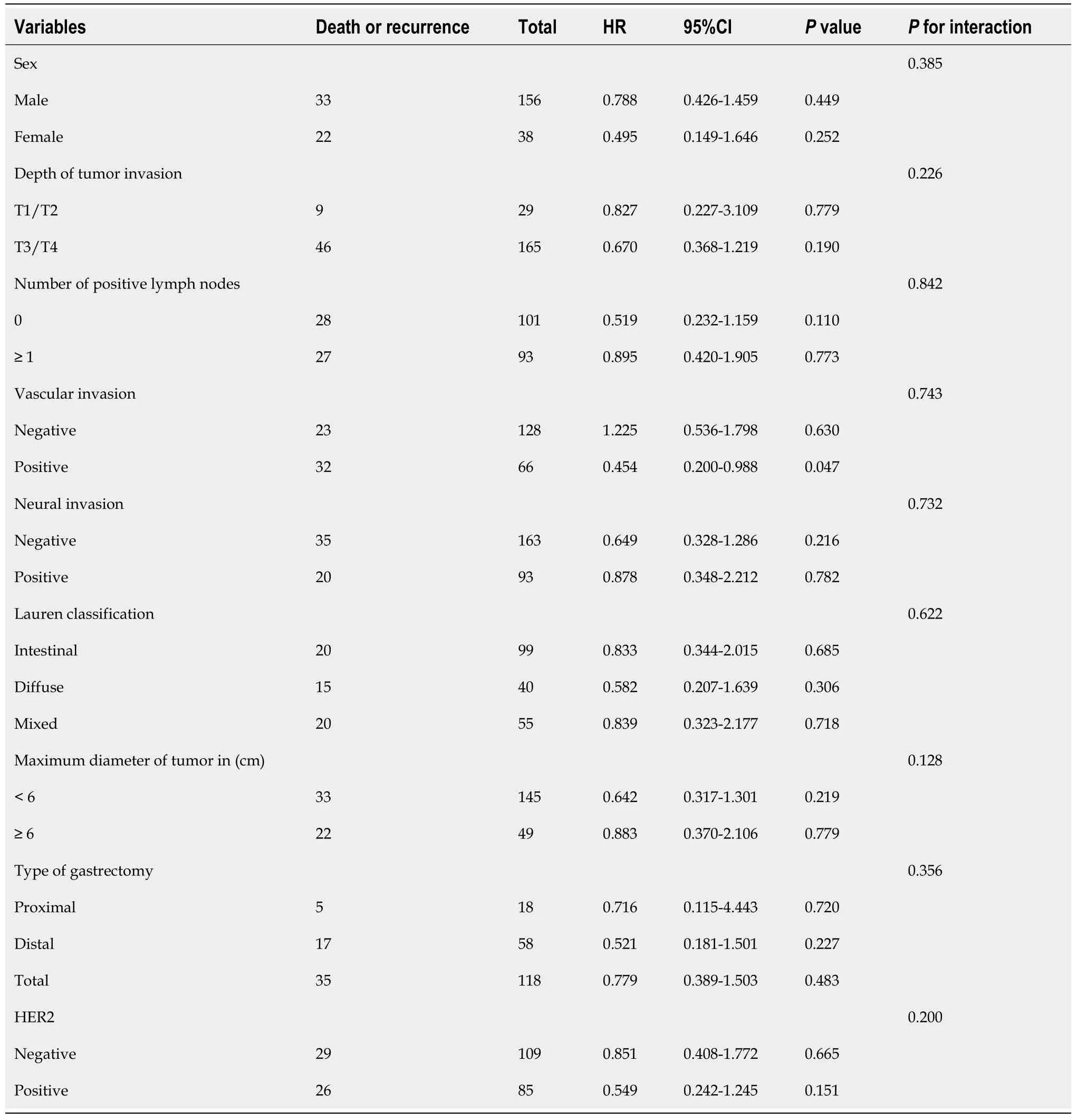
Table 3 Subgroup analysis of progression-free survival by Cox regression analysis of chemotherapy cycles of stage ll gastric cancer
PSM and subgroup analysis of TNM stage III gastric cancer patients
Patients in the < 9 cycles group received the following chemotherapy regimens:(1)5 patients received S-1 + apatinib;(2)4 patients received S-1 + DCF;(3)10 patients received SOX + FOLFOX;(4)4 patients received S-1 + FOLFOX;(5)8 patients received XELOX;(6)98 patients received FOLFOX;and(7)18 patients received multiple regimen combinations.Patients in the ≥ 9 cycles group received the following chemotherapy regimens:(1)142 patients received S-1;(2)2 patients received SOX;(3)2 patients received S-1 + DCF;(4)29 patients received capecitabine;(5)9 patients received doxifluridine;(6)6 patients received SOX + FOLFOX;(7)2 patients received FOLFOX;and(8)50 patients received multiple regimen combinations.Twenty-four patients in the < 9 cycles group and forty-one patients in the ≥ 9 cyclesgroup received neoadjuvant chemotherapy plus adjuvant chemotherapy.Two hundred eighteen patients in the < 9 cycles group and two hundred and one patients in the ≥ 9 cycles group received only postoperative adjuvant chemotherapy.
All patients with TNM stage III(n= 902)were grouped based on nine variables(sex,vascular invasion,nerve invasion,number of positive lymph nodes,depth of tumor invasion,maximum tumor diameter,Lauren classification,type of gastrectomy,and HER2 status)according to the cycles of chemotherapy received(< 9 cyclesvs≥ 9 cycles).Significant differences in age(P< 0.001)and type of gastrectomy(P= 0.044)were observed between the < 9 cycles group and the ≥ 9 cycles group before PSM.After PSM,in which 484 patients were included(there were 242 patients in the ≥ 9 cycle group and 242 patients in the < 9 cycle group),differences were observed between variables in the two groups(P> 0.05).The Hansen and Bowers overall balance test indicated that the distribution between the two groups was well balanced after PSM(Table 4,Figures 4 and 5).
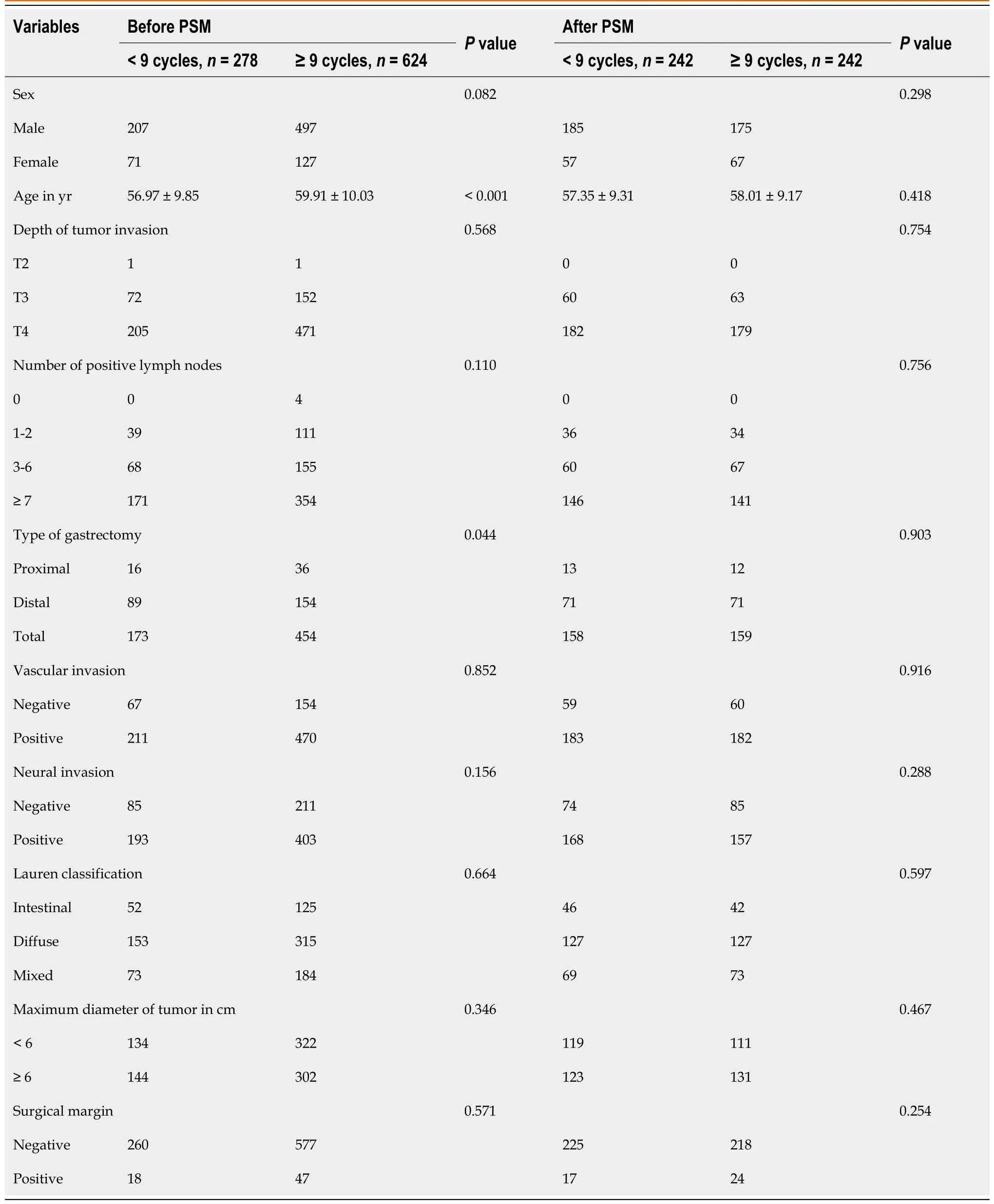
Table 4 Patient characteristics before and after propensity score matching based on the number of chemotherapy cycles for stage lll gastric cancer
OS and PFS were similar in both groups before and after PSM(P> 0.05),indicating that in patients with stage III gastric cancer ≥ 9 chemotherapy cycles does not impart a survival benefit(Figures 4 and 5).In detail,the 1-year OS rate(91.7%vs92.5%,log-rankP= 0.735),3-year OS rate(67.4%vs63.6%,log-rankP= 0.389),and 5-year OS rate(47.1%vs42.5%,log-rankP= 0.315)were not statistically different.The 1-year and 3-year PFS rates in the ≥ 9 period group and the <9 period group were statistically significant(80.1%vs62.0%,log-rankP< 0.001,respectively,and 44.2%vs54.5%,log-rankP= 0.023,respectively).However,that benefit was not observed in the 5-year PFS rate(38.4%vs33.9%,log-rankP= 0.298).We observed that ≥ 9 chemotherapy cycles can significantly reduce the probability of recurrence compared to < 9 chemotherapy cycles(24.4%vs48.8%,respectively,P< 0.001),local-regional metastasis(10.7%vs21.1%,respectively,P= 0.002),and distant metastasis(12.4%vs24.0%,respectively,P= 0.001)but not peritoneal metastasis(1.2%vs3.7%,respectively,P= 0.090).
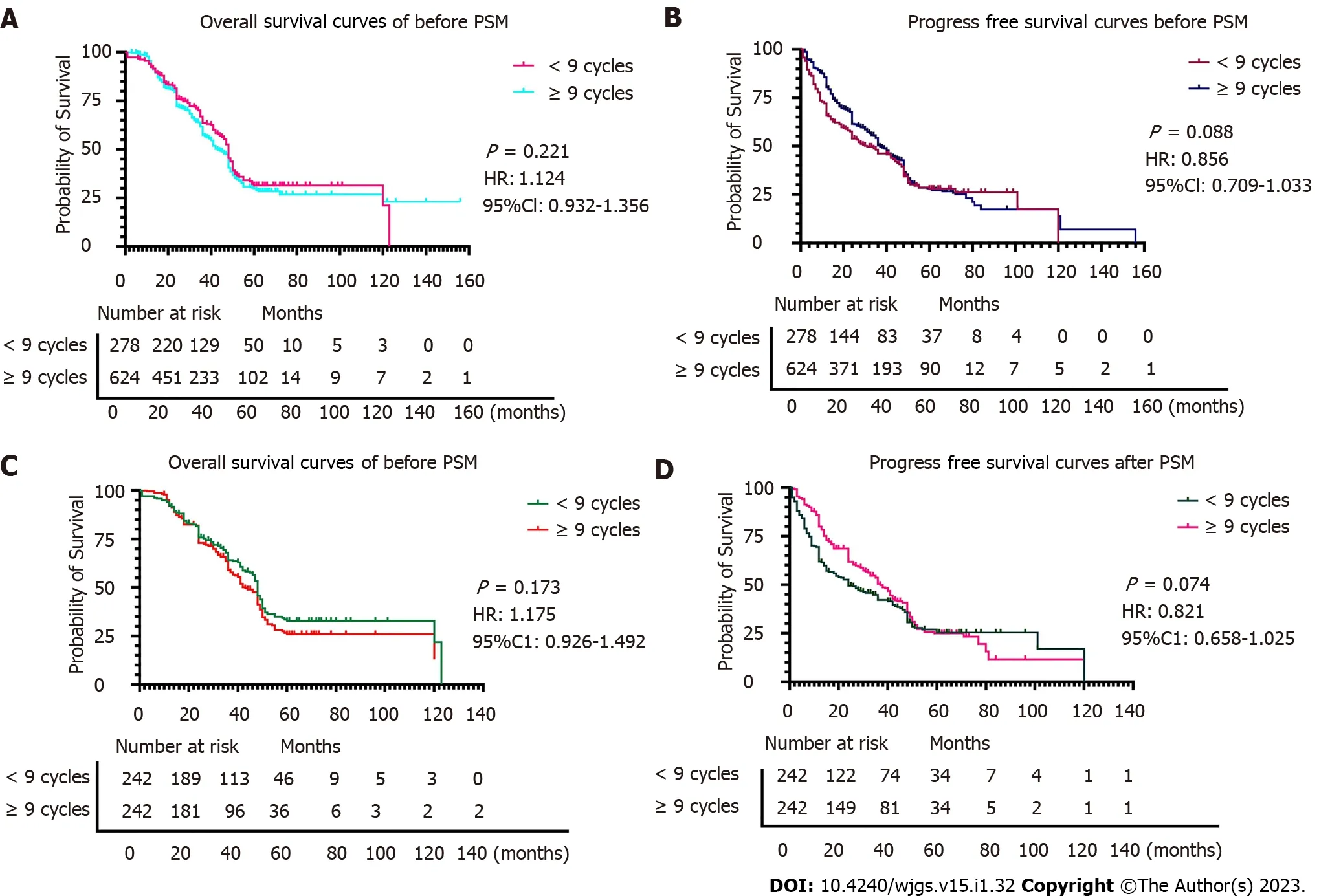
Figure 4 Comparison of overall survival and progression-free survival before and after propensity score matching in stage lll gastric cancer patients.A:Comparison of overall survival between the two groups based on chemotherapy cycles before propensity score matching(PSM);B:Comparison of progression-free survival between the two groups based on chemotherapy cycles before PSM;C and D:Comparison of overall survival(C)and progression-free survival(D)between the two groups based on chemotherapy cycles after PSM.
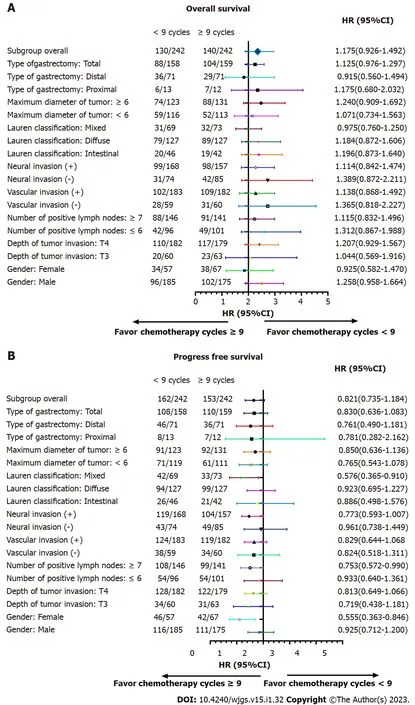
Figure 5 Subgroup analysis of overall survival and progression-free survival for chemotherapy cycles in stage lll gastric cancer patients.A:Subgroup analyses of overall survival based on chemotherapy cycles;B:Subgroup analyses of progression-free survival based on chemotherapy cycles.
We performed subgroup analyses according to depth of tumor invasion,sex,vascular invasion,neural invasion,number of positive lymph nodes,maximum diameter of tumor,Lauren classification,types of gastrectomy,and HER2 in order to determine if a survival benefit of ≥ 9 cycles was evident in specific patient populations.The analyses demonstrated that the ≥ 9 chemotherapy cycles group had increased OS compared to the < 9 chemotherapy cycles for most subgroups(Table 5).Significant interactions were observed between chemotherapy cycles and the number of positive lymph nodes(Pfor interaction = 0.007),Lauren classification(Pfor interaction = 0.002),type of gastrectomy(Pfor interaction = 0.004),and maximum tumor diameter(Pfor interaction < 0.001).
After further interaction subgroup analyses,patients with ≤ 6 positive lymph nodes[hazard ratio(HR):1.312,95% confidence interval(CI):0.867-1.988],with intestinal type(HR:1.196,95%CI:0.873-1.640),receiving proximal gastrectomy(HR:1.175,95%CI:0.680-2.032),with ≥ 6 cm maximum diameter of tumor(HR:1.240,95%CI:0.909-1.692)showing a higher risk of total mortality in the < 9 cycles group compared with the ≥ 9 cycles group(Table 6).
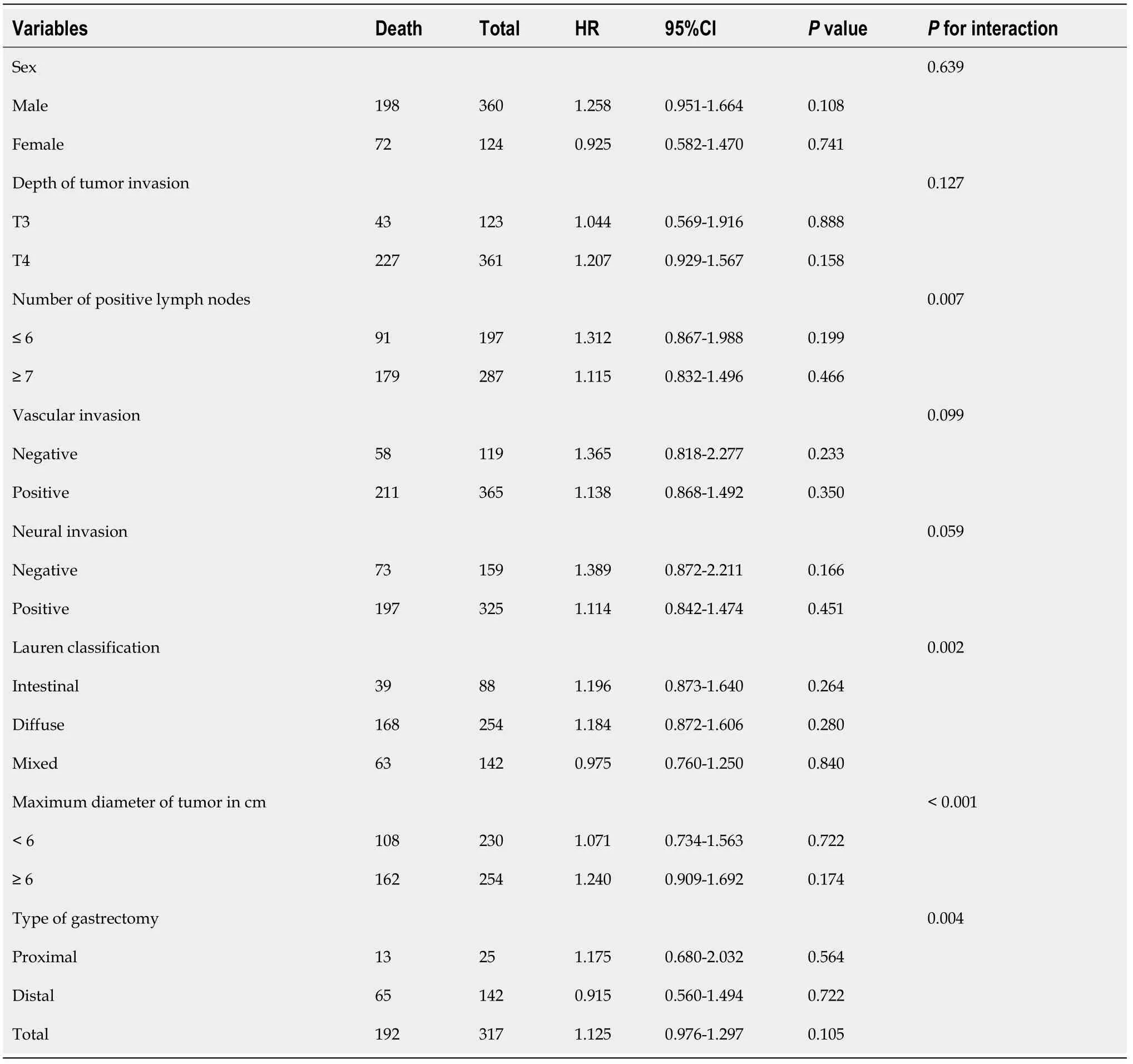
Table 5 Subgroup analysis of overall survival by Cox regression analysis of stage lll gastric cancer patients
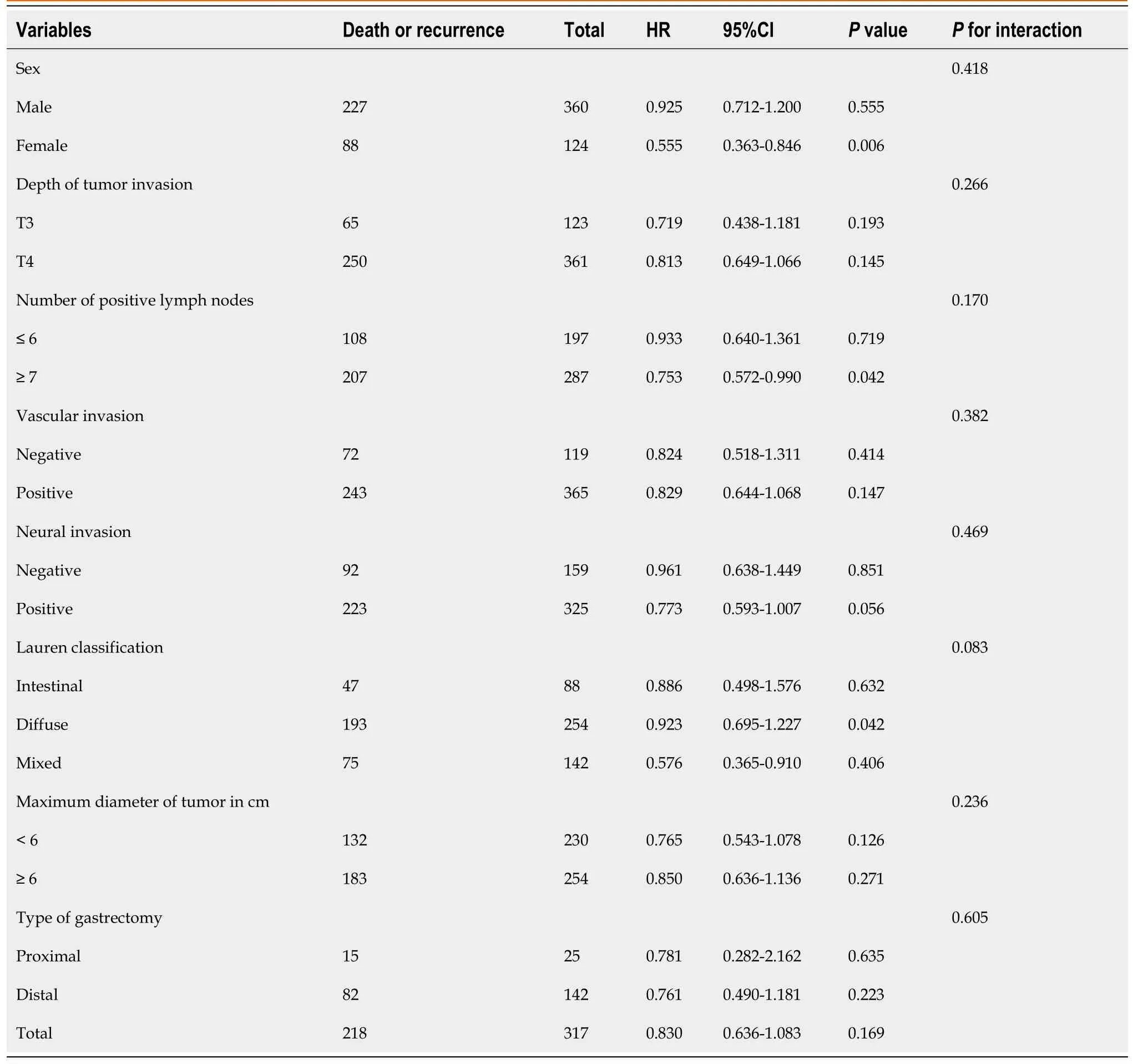
Table 6 Subgroup analysis of progression-free survival by Cox regression analysis of stage lll gastric cancer patients
DlSCUSSlON
According to relevant data,the literature shows that the number of chemotherapy cycles received by patients is associated with the prognosis.A study conducted in China showed that patients with triplenegative breast cancer who received at least four chemotherapy cycles had a significantly better survival rate[8].Another study in China focused on the link between the number of chemotherapy cycles and the survival rate of patients with bone-only metastasis[9].Survival factors and prognostic factors of nasopharyngeal carcinoma patients were explored and analyzed,and the conclusion was drawn that the influencing factors of OS included the number of chemotherapy cycles and the number of metastatic sites.An investigation in Australia showed that the survival rate and pathological response rates of patients with muscle invasive bladder cancer were better in patients receiving 4 cycles of neoadjuvantchemotherapy compared to patients receiving 3 cycles of neoadjuvant chemotherapy[10].A study in China observed that the optimal number of adjuvant chemotherapy cycles for colon cancer patients is often less than 5[11].
While some studies have shown that more cycles of chemotherapy lead to a better prognosis,other studies have demonstrated no effect or a worsened effect.For example,patients with ovarian cancer receiving ≥ 5 chemotherapy cycles had a poorer prognosis than patients receiving 3-4 cycles[12].Another study found that chemotherapy does not reduce survival in patients with inoperable stage III NSCLC.However,increased cycles(3 or more)led to more grade 3 toxicities[13].In addition,a different study conducted on patients with ovarian cancer demonstrated that additional cycles did not affect the recurrence or complete pathologic response[14].The 5-year survival rate of locally advanced rectal cancer treated with chemotherapy was higher than that of untreated patients[15].Finally,patients with colorectal cancer who received adjuvant chemotherapy had a better 3-year survival rate than those who received shorter courses of chemotherapy[16].
Although it seems that increased chemotherapy cycles tend to achieve an oncologic benefit,the data is lacking for gastric cancer.Through a series of studies and analyses,the minimum number of cycles should be completed in gastric cancer patients to reduce the rate of tumor growth.During this process,the researchers found that patients who completed less than four cycles did not have a higher survival rate[17].By analyzing the contents of previous studies,we can see that there is a certain correlation between gastric cancer recurrence and chemotherapy cycle.It was proved that > 9 cycles of che-motherapy could not reduce the recurrence rate of gastric cancer,and there was no advantage.Less than 9 cycles of chemotherapy increased the recurrence rate and reduced OS[18].
In the current study,the data demonstrated that ≥ 9 chemotherapy cycles did not confer any oncological benefit compared to < 9 chemotherapy cycles,indicating that ≥ 9 cycles may be considered overtreatment in stage II gastric cancer patients.Excessive chemotherapy may cause unpleasant side effects and impact the immune system,hepatic function,renal function,etc.However,≥ 9 chemotherapy cycles did significantly reduce the probability of overall recurrence,local-regional metastasis,and distant metastasis rates in stage III gastric cancer patients but did not affect OS or PFS.Excessive chemotherapy cycles may have a psychological effect for patients(i.e.a patient may have less anxiety while being treated despite any side effects).
At present,there are some urgent problems in the research process.First of all,this study mainly conducted retrospective analysis and focused on a single factor.Although PSM was used to reduce the bias,it was still not accurate enough.The purpose of using PSM is to conduct a simulated randomized experiment.Secondly,the chemotherapy regimen is not standardized and complete;therefore,the effects of different chemotherapy regimens were not analyzed.Nonetheless,the interaction effect between chemotherapy cycles and Lauren classification,types of gastrectomy,and maximum diameter of the tumor on OS were determined for the first time.
CONCLUSlON
Overall,patients with stage II and III gastric cancer with chemotherapy cycles ≥ 9 have no significant effect on the prognosis of gastric cancer,so ≥ 9 cycles of chemotherapy are not adopted.However,in essence,≥ 9 cycles of chemotherapy has a certain benefit in reducing the recurrence rate of stage III gastric cancer patients.Due to the lack of relevant data on gastric cancer and chemotherapy cycles at the present stage,it is necessary to complete the chemotherapy regimen in a more standardized way,so as to deepen the research and finally clarify the correlation between the prognosis of gastric cancer and chemotherapy cycles.
ARTlCLE HlGHLlGHTS
Research background
Several studies have shown an oncological benefit with increased cycles of chemotherapy in different cancer types.However,some studies have shown no effect or a worsened effect.
Research motivation
According to a series of exploration and analysis,it is found that there is no abundant data to prove the correlation between the prognosis of gastric cancer and the duration of chemotherapy.
Research objectives
The main purpose of this study is to analyze and explore whether there is a correlation between survival rate and chemotherapy cycle in patients with stage II gastric cancer and stage III gastric cancer.
Research methods
A 1:1 ratio was used in the propensity score matching analysis to reduce the differences between groups with different chemotherapy cycles.Progression-free survival,overall survival and recurrence were components of outcome indicators.
Research results
There was no statistically significant difference in progression-free survival and overall survival between the two groups of stage II and III patients.However,overall recurrence(P< 0.001),localregional metastasis(P= 0.002),and distant metastasis(P= 0.001)in the ≥ 9 chemotherapy cycles group were significantly lower than those in the < 9 chemotherapy cycles group for stage III gastric cancer patients.
Research conclusions
For stage II and III gastric cancer patients,≥ 9 cycles of chemotherapy should not be considered as far as possible,because ≥ 9 cycles of chemotherapy cannot effectively reduce the recurrence rate.
Research perspectives
After a series of studies,it is found that the relationship between the prognosis of gastric cancer and the chemotherapy cycle needs to be further explored to make a more abundant and standardized chemotherapy regimen.
FOOTNOTES
Author contributions:Li YF and Zhang WB conceptualized and designed the study,collected and analyzed the data,and wrote the manuscript;Li YF,Zhang WB and Gao YY revised the manuscript for important intellectual content;Gao YY participated in collection of the data;All authors approved the final version of the manuscript.
lnstitutional review board statement:This study was approved by the Institutional Research Ethics Board of Ethics Committee of Shanxi Cancer Hospital(Taiyuan,China)(No.2022JC23)and followed the Declaration of Helsinki.
lnformed consent statement:All the authors report having no relevant conflicts of interest for this article.
Conflict-of-interest statement:No additional data are available.
Data sharing statement:The authors have read the STROBE Statement - checklist of items,and the manuscript was prepared and revised according to the STROBE Statement - checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Yi-Fan Li 0000-0002-6378-7635.
S-Editor:Liu GL
L-Editor:Filipodia
P-Editor:Liu GL
 World Journal of Gastrointestinal Surgery2023年1期
World Journal of Gastrointestinal Surgery2023年1期
- World Journal of Gastrointestinal Surgery的其它文章
- Hereditary polyposis syndromes remain a challenging disease entity:Old dilemmas and new insights
- Application of ablative therapy for intrahepatic recurrent hepatocellular carcinoma following hepatectomy
- Postoperative adjuvant therapy for hepatocellular carcinoma with microvascular invasion
- Development and validation of a novel nomogram for predicting overall survival in gastric cancer based on inflammatory markers
- New perspectives on robotic pancreaticoduodenectomy:An analysis of the National Cancer Database
- lmpact of body mass index in elderly patients treated with laparoscopic liver resection for hepatocellular carcinoma