
Male masturbation device for the treatment of premature ejaculation
2016-06-07 09:42:55RodrguezJEpezAInstitutoSexolgicoMurciano
Rodríguez JE, L?pez AInstituto Sexol?gico Murciano
ABSTRACT
Objective:To determine the efficiency as a treatment of the first line masturbator aid device for patients with premature ejaculation (PE). Methods:A whole of 18 cases with lifelong PE used a masturbator TENGA, 5 times per week for 6 weeks and a minimum of 5 minutes for every use. Premature Ejaculation Profile (PEP) was used to measure the effects of its use. As a main outcome measure were used the proportion of patients who achieved criteria for clinical benefit, defined as achieving a two-category or greater increase in the change in control over ejaculation and level of satisfaction with intercourse, and a one-category or greater increase in the change in ejaculation-related distress and degree of interpersonal difficulty. Results:The proportion of man who achieved the criteria for clinical benefit were 83 % in control over ejaculation during sexual intercourse, 72% in ejaculation distress and interpersonal difficulties and men’s lower proportion met criteria was in satisfaction with sexual intercourse (33%). Conclusions:The patients who used the device Flip Hole increased of significant form the control grade on the ejaculation, and its interpersonal ejaculation distress and they reduced difficulties. To further evaluate the validity of these claims, randomized controlled trials should occur.
ARTICLE INFO
Article history:
Received 27 March 2015
Received in revised form 10 September 2015 Accepted 15 September 2015
Available online 1 January 2016
?
Male masturbation device for the treatment of premature ejaculation
Rodríguez JE*, L?pez A
Instituto Sexol?gico Murciano
ABSTRACT
Objective:To determine the efficiency as a treatment of the first line masturbator aid device for patients with premature ejaculation (PE). Methods:A whole of 18 cases with lifelong PE used a masturbator TENGA, 5 times per week for 6 weeks and a minimum of 5 minutes for every use. Premature Ejaculation Profile (PEP) was used to measure the effects of its use. As a main outcome measure were used the proportion of patients who achieved criteria for clinical benefit, defined as achieving a two-category or greater increase in the change in control over ejaculation and level of satisfaction with intercourse, and a one-category or greater increase in the change in ejaculation-related distress and degree of interpersonal difficulty. Results:The proportion of man who achieved the criteria for clinical benefit were 83 % in control over ejaculation during sexual intercourse, 72% in ejaculation distress and interpersonal difficulties and men’s lower proportion met criteria was in satisfaction with sexual intercourse (33%). Conclusions:The patients who used the device Flip Hole increased of significant form the control grade on the ejaculation, and its interpersonal ejaculation distress and they reduced difficulties. To further evaluate the validity of these claims, randomized controlled trials should occur.
ARTICLE INFO
Article history:
Received 27 March 2015
Received in revised form 10 September 2015 Accepted 15 September 2015
Available online 1 January 2016
Keywords:
Premature ejaculation
Masturbation
Treatment
Device
Premature ejaculation profile questionnaire
E-mail:jesuseugenio@isemu.es
1. Introduction
The premature ejaculation is the most frequent sexual malfunction in the world, the predominance valuations has changed a lot, nevertheless it is believed that 15 % of men would present symptoms compatible with PE [1-5].
Different subtypes have been postulated and etiologist for the PE, from the first explanations of psychological cut based on inadequate learning associated at high levels of anxiety, up to the last hypotheses neurobiological that postulate a possible hyposensibility of the recipients 5-HT2C and hypersensitivity of 5-HT1A like cause of the PE. The true thing is that there is today none of these explanations has assembled sufficiently empirical support.
As for the available treatments it is undoubtedly the pharmacotherapy that I support empirically has until now emphasizing the use of selective serotonin reuptake inhibitors (SSRI’s) [6, 7], and tramadol [8], and in a background the use of topical local anaesthetics [9], phosphodiesterase type 5 inhibitors (PDE5i) [10], and alpha-adrenergic blockers [11]. For his part the psychological treatments of cognitive cut - behavioural keep on being used and turn out to be effective in spite of the scarce empirical support [12-14].
In general, the patients with PE would obtain the biggest clinical benefit with the combination of ISRS and a cognitive - behavioural therapy [7, 15]. This combination corrects certain limitations that present both treatments separately. Nevertheless the accessibility to this treatment is very limited, also, the cost, the side effects and the need for collaboration on the part of the couple does that many men could not benefit from the same one. New treatment lines are necessary therefore for these men that they complement the arsenal therapeutic available.
In this sense, at least two independent groups in Japan have putt TENGA products to clinical usage. One of them have applied Tenga for ejaculatory disorders [16] and the other have used TENGA on tonumber of patients suffering from intravaginal anejaculation or postprostatectomy dysfunction [17].
TENGA is a Japanese brand of masturbation aids produced by the company of the same name. Masturbation aids (masturbators), personal lubricants, and other related products are sold under this brand. The hypothesis is that, if an organ is hypersensitive, an increase rather than a decrease in the intensity and frequency of stimulation should result in habituation. This cases series examines the possible clinical benefit of using device Flip Hole in PE patients in the absence of therapeutic contact and couple collaboration.
In Spain, concretely in the Region of Murcia, we have found studies that use a device masturbation aid as treatment for the PE. The aim of this study was to assess the efficacy of a masturbator aid device for the treatment of patients with PE in an individual format and answer Jan Wise, Watson′s study [18] and J.E. Rodríguez, A. López study [19].
2. Material and methods
After several weeks of announcements in press, radio and social networks, we had received 30 requests of participation in the study. After the first interview in which there was applied to them Premature Ejaculation Diagnostic Tool (PEDT), 10 patients were pushed back because they were not fulfilling the criteria (to come at least to a punctuation of 11), to the rest they were called for the second time and I request them a battery of analytical tests, after they are examined the same an autorecord of the estimated intravaginal ejaculatory latency was delivered to him steal (IELT) that they had to refill for two weeks, also the MCMI-III is administered to them and they signed an informed assent.
The inclusion criteria were:Participants must be heterosexual males and in a stable monogamous, sexual relationship with a female partner for at least 6 months, must score =11 in the Premature Ejaculation Diagnostic Tool (PEDT), must have a selfestimated average intravaginal ejaculatory latency time (IELT) of <2 minutes, must be in good general health with no clinically significant abnormalities as determined by medical history, and clinical lab results.
The exclusion criteria were:To suffer an alteration or mental disorder according to the criteria of the DSM-IV, history of alcohol abuse and dependence, do not to consume medication, drugs of recreative use or alcohol (except for caffeine or nicotine/tobacco).
Spent two weeks there was a third interview in which the averages of the IELT were verified, 20 patients were fulfilling the criteria established for the IELT, then they completed the Premature Ejaculation Profile (PEP), then, it was time when device Flip Hole is delivered to them (Figure 1) and to high quality lubricant called TENGA hole lotion really, after realizing a demonstration of how it was used, one gave them the following use rules for 6 weeks. “During the next six weeks you will use this devices without partner and at least 5 times per week, in every use you will be at least 5 minutes masturbating with the lubricated device, if you see that you are going to ejaculate earlier, for and one waits moments until you could continue up to 5 minutes”. In this moment , they signed a new informed assent.
During the following 6 weeks there was maintained contact by e-mail and by phone, at least once for week to verify that the instructions were following and to solve doubts or any incidence with the use of the device.
Spent 6 weeks they were called for another interview, of 20 patients 18 had used the device a minimum of 5 occasions per week and they respected the minimal use times, 2 patients did not come at the interview. Is applied to them again Premature Ejaculation Profile (PEP).
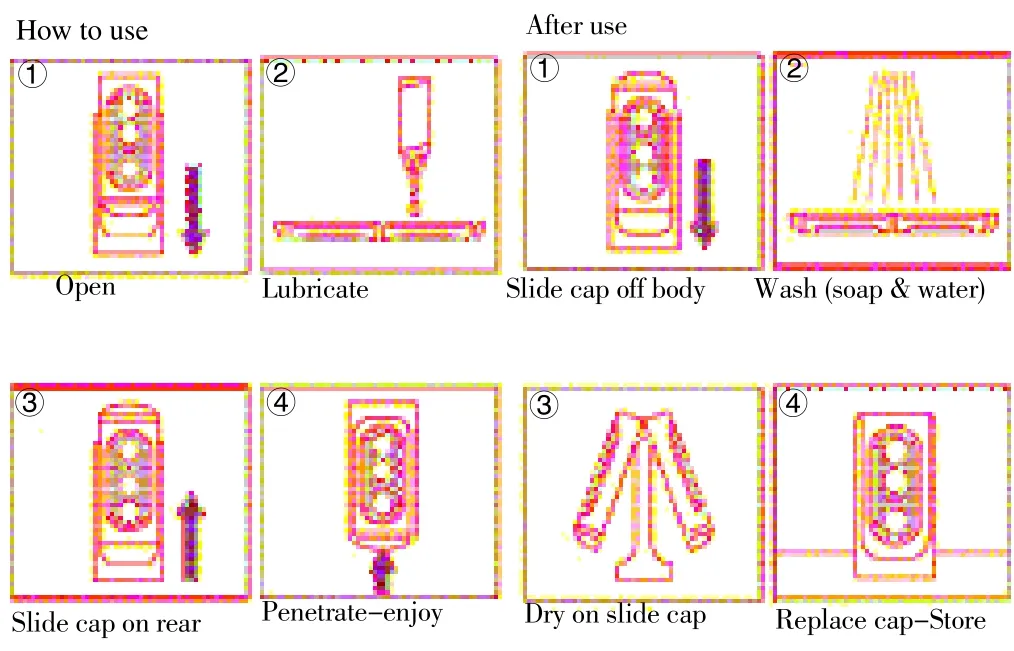
Figure 1. Flip Hole device (Size 85×68×175 mm/558 g).The Flip Hole features a hard case with flexible front face and buttons. Inside soft elastomer shapes hypoallergenic.
The PEP is a validated self-report questionnaire used to assess the four measures of PE defined by the DSM-IV-TR:satisfaction with sexual intercourse, control over ejaculation, ejaculation-related distress, and interpersonal difficulty. Each measure regarding ejaculation is scored on a 5-point scale.
As a main outcome measure were used the proportion of patients who achieved criteria for clinical benefit. Criteria for clinical benefit were defined as achieving a two-category or greater increase in the change in control over ejaculation and level of satisfaction with intercourse , and a one-category or greater increase in the change in ejaculation-related distress and degree of interpersonal difficulty, at the study end point compared with baseline values [20-22].
3. Results
Of the whole of 20 patients that overcame the first phase only 18 patients completed the study. The median age at the study end point was 27 (range 20-42). Lifelong PE was diagnosed in 18 men (100%). Men who had been in a stable, monogamous, heterosexual relationship with the same partner for at least 6 months represented 100% whereas those married comprised 33.3 %. All participants came from Murcia city.
Criteria for clinical benefit were defined as achieving a twocategory or greater increase in the change in control and satisfaction and a one-category or greater increase in the change in distress and interpersonal difficulty.
A significantly higher proportion of men met the criteria for clinical benefit with the use of the device, the higher proportion of man who achieved the criteria was in control over ejaculation during sexual intercourse (15, 83%). The proportion of man who achieved the criteria in ejaculation distress and interpersonal difficulty were both 72% (13), and men’s lower proportion met criteria was in satisfaction with sexual intercourse (6, 33%). No side-effect, no pains was reported associated with use of the device.
4. Discussion
The results of this study of series of cases demonstrates that the ruled use of the device Flip Hole might be used like a treatment of the first effective line of the PE, since it generated a significant increase of the control ejaculatory, and interpersonal distress and reduced clearly the personal ejaculation-related difficulty in the men who used it.
This clear progress might owe to the combination of the physical characteristics of the device Flip Hole associated with the rules of masturbation that the patients continued. Although the theories that PE and hypersensitivity defends association between are in the low hours. The sensitivity of the glans penis, the organ triggering ejaculatory reflex, undoubtedly has an important role in the ejaculatory mechanism. The physical characteristics of the Flip Hole device produces to stimulation of glans penis very intense, continue and with similarities to the vaginal introit, this stimulation you prop it would happen in conditions where the man is not sexual performance anxiety being able to identify better the sensations that precede the orgasm, at the same time we believe that it was possible to generate a desensitization effect in the Nervous System for the use repeated given the intense of the stimulus.
In relation to the treatments of the first line that we arrange the use of this device it presents three big advantages, the first one who does not need the collaboration on the part of the couple, the second one who lacks side effects and the third one that it is not necessary to come to the consultation of a specialist for its use. This device would represent a good therapeutic option for those men without stable couple or who cannot gain access to costly therapies, or are recover to take an ISRS, or the side effects of the same are not tolerated, and especially for this majority group of men who are opposite to coming to the specialist[3].
The device for the treatment of PE described in this article appears like to promising new first line treatment for Premature Ejaculation, with clear advantages on the available treatments up to the date as regards costs, accessibility, facility of use and rapidity in the progress, and it would not have side effects.
The main limitation of the study is the number of cases; it is very small to draw a solid conclusion for such to common sexual problem (PE). Also the lack of control group and long term follow up are limitations of the study since we cannot know how long the progress stays obtained once it stops being used.
The ruled use of the device Flip Hole for 6 weeks has collaborated with a significant increase of the control ejaculatory as well as to a reduction of the ejaculation-related personal distress levels and interpersonal difficulty for PE in the men who took part in the study. These facts make us consider being the use of the device Flip Hole a possible new treatment of the first for the Premature Ejaculation. To further evaluate the validity of these claims, randomized controlled trials should occur.
Conflict of interest statement
The authors report no conflicts of interest.
Acknowledgments
The authors would like to thank Julian Vigara, Eva Camacho and Pedro Tripiana for their collaboration in the trial, and Ana Fuentes and Lola Clares for their assistance in the development of this manuscript. We would also like to thank to Tenga Corporation for their device.
References
[1] Althof S, Abdo C, Dean J, Hackett G, McCabe M, McMahon C, et al. International Society for Sexual Medicine’s Guidelines for the diagnosis and treatment of premature ejaculation. J Sex Med 2010; 7:2947-69.
[2] McMahon CG, Althof SE, Waldinger MD, Porst H, Dean J, Sharlip ID, et al. An evidence-based definition of lifelong premature ejaculation:report of the International Society for Sexual Medicine (ISSM) ad hoc committee for the definition of premature ejaculation. J Sex Med 2008; 5:1590-606.
[3] Carson C, Gunn K. Premature ejaculation:definition and prevalence. Int J Impot Res 2006; 18:S5-13.
[4] Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, et al. Guidelines on male sexual dysfunction:Erectile dysfunction and premature ejaculation. Euro Urol 2010:epub. doi:10.1016/j.eururo.2010.02.020.
[5] Waldinger M. The neurobiological approach to premature ejaculation. J Urol 1998; 168:2359-2367.
[6] Waldinger M, Berendsen HH, Blok BF, Olivier B, Holstege G. Premature ejaculation and serotonergic antidepressants-induced delayed ejaculation:the involvement of the serotonergic system. Behav Brain Res 1998; 92:111-118.
[7] Yuan P, Dai J, Yang Y, Guo J, Liang R. A comparative study on treatment for premature ejaculation:citalopram used in combination with behavioral therapy versus either citalopram or behavioral therapy alone [Chinese]. Chin J Androl 2008:22:35-38.
[18 Kaynar M, Kilic O, Yurdakul T. On-demand tramadol hydrochloride use in premature ejaculation vtreatment. Urology 2012; 79:145-149.
[9] Dinsmore WW, Hackett G, Goldmeier D, Waldinger M, Dean J, Wright P, et al. Topical eutectic mixture for premature ejaculation TEMPE):a novel aerosol-delivery form of lidocaine-prilocaine for treating premature ejaculation. BJU Int 2007; 99:369-375.
[10] Aversa A, Pili M, Francomano D, Bruzziches R, La pera G, Spera G, et al. Effects of vardenafil administration on intravaginal ejaculatory latency time in men with lifelong premature ejaculation. Int J Impot Res 2009; 21:221-227.
[11] Cavallini G. Alpha-1 blockade pharmacotherapy in primitive psychogenic premature ejaculation resistant to psychotherapy. Eur Urol 1995; 28:126-130.
[12] Semans J. Premature ejaculation. Southern Med J 1956:49:352-358.
[13] Masters WH, Johnson VE. Human sexual inadequacy, Boston:Little Brown; p. 1970.
[14] Kaplan HS. The new sex therapy, New York:Brunner/Mazel;p.197.
[15] Tang W, Ma L, Zhao L, Liu Y, Chen Z. Clinical efficacy of Viagra with behavior therapy against premature ejaculation. Zhonghua Nan Ke Xue 2004:10:3667-3670.
[16] Yoshitomo K. Rehabilitation for severe delayed ejaculation (intravaginal ejaculation disorder) with use of a masturbation aid. Asian Pac J Reprod 2012; 1(4):262-2648.
[17] Yoshitomo Kobori, Ryo Sato, Yoshio Ashizawa, Hiroshi Yagi, Shigehiro So, Gaku Arai, et al. Mullerian duct cyst:a curable entity of male infertility, two case reports. Reprod Med Biol 2009; 24 (3):355-357.
[18] Jan Wise ME, Watson JP. A new treatment for premature ejaculation:Case series for a desensitizing band. Sex Relation Ther 2000;15:4,345-350.
[19] McMahon C, Kim SW, Park NC, Chang Chin-pao, Rivas D, Tesfaye F, et al. Treatment of premature ejaculation in the Asia-Pacific region:results from a phase III double-blind, parallel-group study of dapoxetine. J Sex Med 2010; 7:256-268.
[20] Patrick DL, Giuliano F, Ho KF, Gagnon DD, McNulty P, Rothman M. The premature ejaculation profile:validation of self-reported outcome measures for research and practice. BJU Int 2009; 103:358-364.
[21] Buvat J, Tesfaye F, Rothman M, Rivas DA, Giuliano F. Dapoxetine for the treatment of premature ejaculation:results from a randomized, double-blind, placebo-controlled phase 3 trial in 22 countries. Eur Urol 2009;55:957-968.
[22] Kaufman JM, Rosen RC, Mudumbi RV, Tesfaye F, Hashmonay R, Rivas D. Treatment benefit of dapoxetine for premature ejaculation:results from a placebo-controlled phase III trial. BJU Int 2009; 103:651-658.
[23] Rodríguez JE, López A. A new treatment for premature ejaculation? Case series for a desensitizing masturbation aid. Asian Pac J Reprod 2015; 1(4):74-77.
doi:Document heading 10.1016/j.apjr.2015.12.015
*Corresponding author:Jes?s Eugenio Rodríguez Martínez. Instituto Sexológico Murciano. C/ Periodista Encarna Sánchez, 22, 030007 Murcia, Espa?a. Tel:868941418
 Asian Pacific Journal of Reproduction2016年1期
Asian Pacific Journal of Reproduction2016年1期
- Asian Pacific Journal of Reproduction的其它文章
- Diagnostic and decision-making difficulties:Placenta accreta at nine weeks’gestation
- Risk factors and adverse perinatal outcomes associated with low birth weight in Northern Tanzania:A registry-based retrospective cohort study
- Analysis of the androgen receptor CAG repeats length in Iranian patients with idiopathic non-obstructive azoospermia
- Returning of cyclicity in infertile Corriedale Sheep with natural progesterone and GnRH based strategies
- Effect of cooling to different sub-zero temperatures on boar sperm cryosurvival
- Milk supplements in a glycerol free trehalose freezing extender enhanced cryosurvival of boar spermatozoa