
Trends and sex differences in atrial fibrillation hospitalization and catheter ablation at tertiary hospitals in China from 2013 to 2016
2022-05-06 08:32:22KangLIFangFangFANPengFeiSUNJieJIANGJingZHOUYingSHIHaiBoWANGJianPingLIYanZHANGYongHUO
Journal of Geriatric Cardiology 2022年4期
Kang LI, Fang-Fang FAN, Peng-Fei SUN, Jie JIANG, Jing ZHOU, Ying SHI, Hai-Bo WANG, Jian-Ping LI, Yan ZHANG,?, Yong HUO,?
1. Department of Cardiology, Peking University First Hospital, Beijing, China; 2. Scientific Project Department, China Standard Medical Information Research Centre, Shenzhen, China; 3. Clinical Trial Unit, the First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China
ABSTRACT BACKGROUND Catheter ablation for atrial fibrillation (AF) is commonly performed worldwide. However, the clinical characteristics of hospitalized patients with AF and national trends in catheter ablation at tertiary hospitals in China remain unreported. METHODS This study used the Chinese national database (Hospital Quality Monitoring System) from 2013 to 2016, which is a mandatory database that collects the front page of patients’ medical records for hospital accreditation, to describe the clinical characteristics of patients with AF as an overall cohort and as subgroups divided by catheter ablation and sex. RESULTS Of 597,919 AF patients first admitted, 57,983 patients underwent catheter ablation [56,384 cases (97.2%) of radiofrequency ablation and 1599 cases (2.8%) of cryoablation]at 746 tertiary hospitals. Nearly 10% of patients hospitalized with AF at tertiary hospitals in China underwent catheter ablation, and the percentage of patients undergoing catheter ablation was on the rise between 2013 and 2016, and the number of cases increased by 2.5 times. Compared with AF patients who did not undergo catheter ablation, those who did were younger, more frequently male, and had fewer baseline comorbidities. Although the overall CHA2DS2-VASc score revealed over half of the patients were high-risk, patients who underwent catheter ablation were mostly low-risk(71.2% of males and 59.1% of females). Considering in-hospital adverse events, the overall pericardial tamponade and all-cause death incidences were 0.2% (0.6% in the ablation group) and 1.2% (0.1% in the ablation group), respectively; both of which were higher in females than males. CONCLUSIONS In this study, AF patients who underwent catheter ablation were relatively young, had a low thrombosis risk,and had few comorbidities and adverse events. Females were older and experienced more complications than males.
Atrial fibrillation (AF) is the most common arrhythmia, with an incidence of 2% in unselected European and North American populations.[1]The incidence of AF increases dramatically with age and comorbidities. A national survey in China involving 31,230 adults aged over 35 years showed that AF incidence was 0.71%.[2]The number of patients with AF is estimated to increase to 5.2 million and 3.1 million for men and women, respectively, in China by 2050.[3]Thus, the disease burden of AF is a significant public health issue in China. AF can lead to a decline in quality of life, increased stroke risk, worsened heart failure (HF), and increased all-cause mortality.
Catheter ablation is a safe and effective method to treat AF. Therefore, catheter ablation has become a routine procedure in patients with AF to improve symptoms and quality of life by reducing the burden of arrhythmia.[4-6]This technology has evolved over the past 20 years and is now commonly performed worldwide. A large retrospective study that used the National Inpatient Sample database in the United States evaluated patients who underwent catheter ablation for AF from 2004 to 2013. The study included 85,977 patients, 32.4% of whom were female. There was no mortality difference between the sexes, but females had higher major and minor complication rates than males.[7]In another study, the researchers identified 50,969 catheter ablation procedures for AF during the study period (2011?2014). They concluded an in-hospital mortality rate of 0.15% and an overall complication rate of 5.46%.[8]In China, catheter ablation for AF has been performed mainly at tertiary hospitals, the highest-ranking medical institutions, in the past 10-20 years. However, the clinical characteristics of patients hospitalized with AF have been scarcely reported, and national trends in AF catheter ablation at tertiary hospitals in China have not been reported. Thus, this study aimed to explore the trends in AF hospitalization and catheter ablation at tertiary hospitals in China from 2013 to 2016.
METHODS
Data Sources
Data were obtained from the Chinese national database, the Hospital Quality Monitoring System (HQMS),a mandatory patient-level national database that collects the front page of patients’ medical records for hospital accreditation.[9-11]Since 2013 in China,tertiary hospitals have been requested to submit standardized electronic inpatient discharge records daily to the HQMS.
Information on demographic characteristics, clinical diagnoses, treatment procedures, and expenditure breakdowns were extracted from the standardized discharge summary known as the “front page” of hospital medical records. Adult patients diagnosed with AF at the cardiology wards of 746 tertiary hospitals with continuously uploaded data between 2013 and 2016 were included in this analysis. Records with missing data on sex, age, and living status at discharge were excluded (Figure 1). For patients with more than one record, only data on the first hospitalization in the same year during this period were included.
This study was authorized by the HQMS Committee Board and approved by the Ethics Committee of Peking University First Hospital (No.2019-93). Furthermore, the requirement for informed consent was waived due to the retrospective research design of this study.
Definition of AF, Catheter Ablation, and Comorbidities
Diagnoses were coded based on the International Classification of Diseases-10 (ICD-10) using certified codes at each hospital. AF and comorbidities were identified using three ICD codes: Beijing RC 020-ICD-10 version, national clinical edition 1.1, and National RC020-ICD-10 version. In addition, two sets of ICD codes identified catheter ablation for AF and pericardial tamponade requiring pericardiocentesis:the Beijing RC022-ICD-9 version of the operation code and the national clinical edition 1.1 of the operating classification code.
Statistical Analysis
Data were analyzed in subgroups according to age(18-34 years, 35-44 years, 45-54 years, 55-64 years,65-74 years, and ≥ 75 years), sex, and use (or not) of catheter ablation. Categorical data are presented as counts (percentages) and were compared with Pearson’s chi-squared test. Continuous data are presented as mean ± SD and were compared with the independent Student’st-test. Statistical analyses were twosided, and aP-value < 0.05 was considered statistically significant. All analyses were performed using R software (version 3.4.3, http://www.R-project.org).
RESULTS
Of the 996 hospitals covered in the HQMS database during the study period, 746 hospitals continued to upload data. Thus, of 597,919 first admissions in which AF was diagnosed at cardiology wards in the same year, we identified 57,983 patients who underwent AF catheter ablation [56,384 cases (97.2%) of radiofrequency ablation and 1599 cases (2.8%) of cryoablation]from January 2013 to December 2016(Figure 1). In the meantime, nearly 10% of patients hospitalized with AF at tertiary hospitals in China underwent AF catheter ablation. However, during this period and within these 746 hospitals, 6.5% of patients with AF catheter ablation were found to receive redo procedures.
The number of AF patients who underwent catheter ablation increased by almost 2.5 times from 8403 to 20,639 per year in China. During this period,the proportion of patients hospitalized with AF at cardiology wards and the percentage of patients undergoing catheter ablation were on the rise (Figure 2).
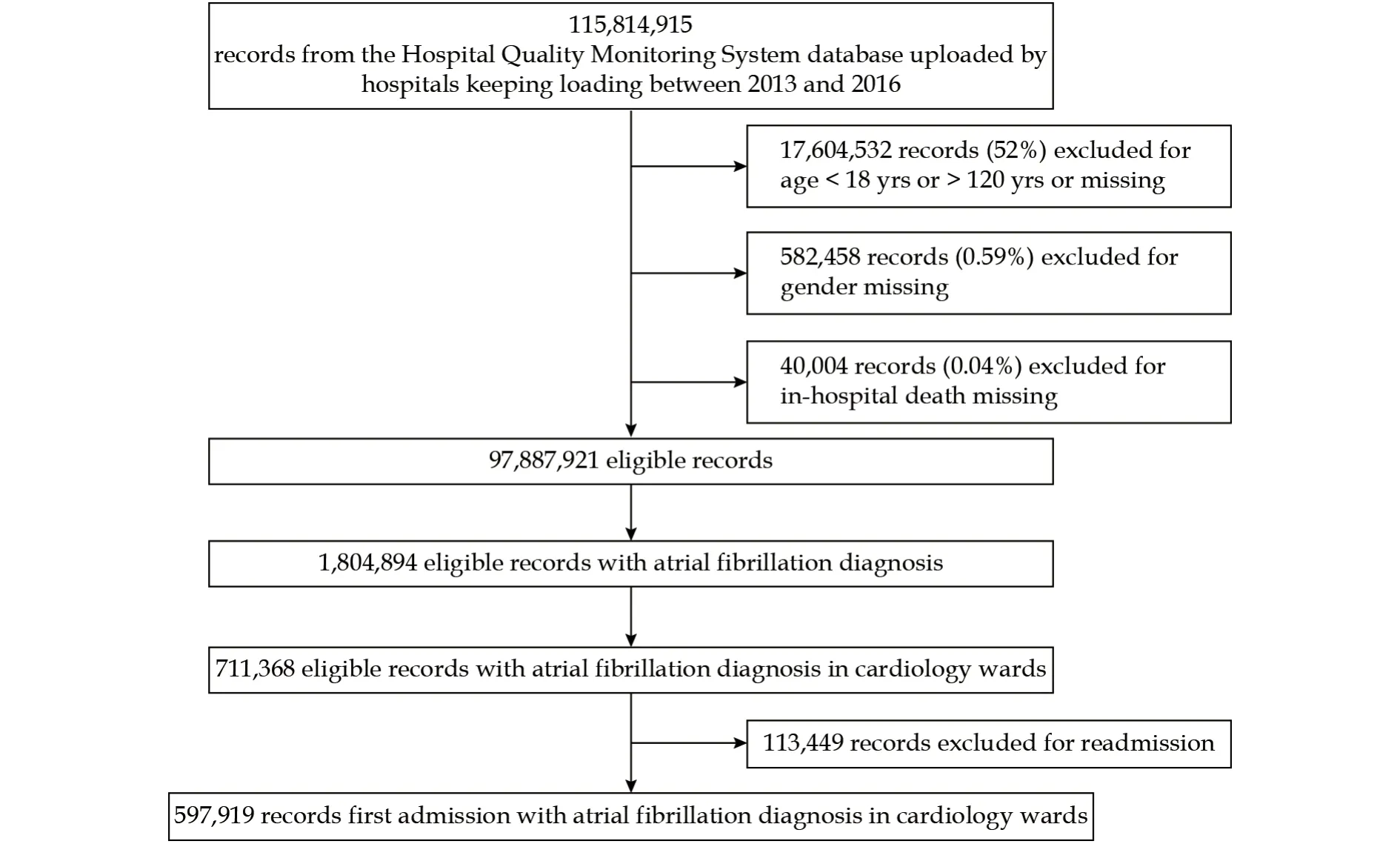
Figure 1 Flow chart of this study.
Types of AF
Although a considerable number of cases on the front page of medical records did not indicate the type of AF (unclassified AF), catheter ablation for AF in China from 2013 to 2016 was still dominated by nonvalvular-related (97.3%) paroxysmal AF (at least 55.9%).
Age Difference and Sex Distribution
The mean age of patients was 68.74 ± 12.03 years,and 46.6% of patients were female. Compared with patients who did not undergo catheter ablation, those who did undergo catheter ablation were younger(59.47 ± 11.12 yearsvs.69.74 ± 11.70 years,P< 0.001)and less frequently female (36.4%vs.47.7%,P< 0.001)(Table 1).
The majority of patients (96.5%) were 45-75 years.However, the age distribution differed according to whether or not catheter ablation was performed (P<0.001). The prevalence of older patients in the ablation group was lower compared with the non-ablation group (27.3%vs.30.4% for patients aged 65-74 years, 7.3%vs.39.2% for patients aged ≥ 75 years).Meanwhile, the patients with AF who underwent catheter ablation were younger. The prevalence of younger patients (aged 18-44 years) was higher in the ablation group than in the non-ablation group (9.8%vs.2.9%,respectively).
The age distribution of patients differed according to sex (P< 0.001). Overall, the female group had a higher proportion of older patients than the male group (31.3%vs.29.1% for patients aged 65-74 years,40.9%vs.32.0% for patients aged ≥ 75 years). This distribution was similar between patients with and without catheter ablation. In the ablation group, females were much older than males, with an average age difference of nearly five years (males: 57.92 ± 11.36 years, females: 62.19 ± 10.11 years;P< 0.001), and the age distribution was significantly right-skewed in the female group compared with the male group(Table 2).
C HA2DS2VASc Thrombotic Risk Score Distribution and Sex Differences
The criterion of high-risk thrombosis was fulfilled if CHA2DS2VASc thrombotic risk score was ≥ 2 for males and ≥ 3 for females.[12]Although the thrombus scores for more than half of the total cohort were high-risk, the score distribution in patients who underwent catheter ablation was quite different from those who did not. Most patients with AF who underwent catheter ablation were at a lower risk of thrombosis. Among the ablation group, the proportion of male patients with a high risk of thrombosis was 28.8% and 69.1% in the ablation group and non-ablation group, respectively (P< 0.001), while the proportion of female patients with a high risk of thrombosis was 40.9% and 75.2%, respectively (Figure 3).
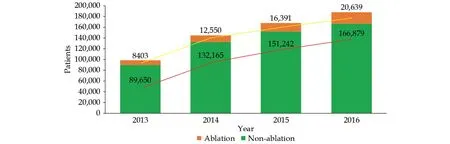
Figure 2 The proportion of hospitalized patients with atrial fibrillation who underwent catheter ablation from 2013 to 2016.
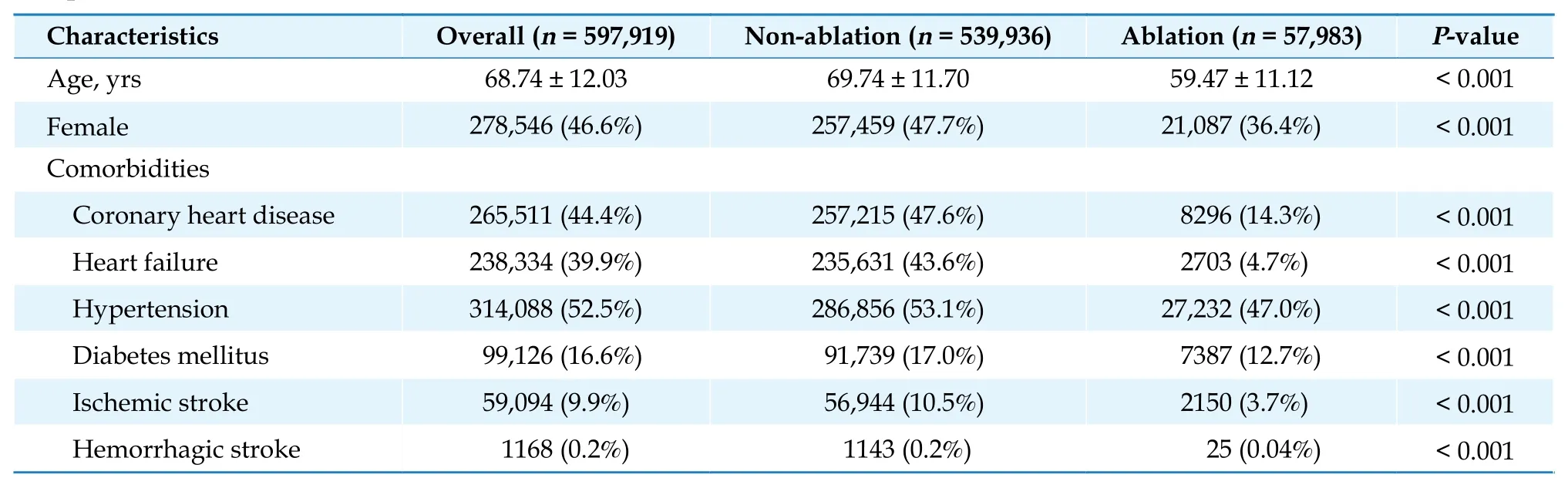
Table 1 Clinical characteristics of all hospitalized patients with atrial fibrillation according to whether or not catheter ablation was performed.
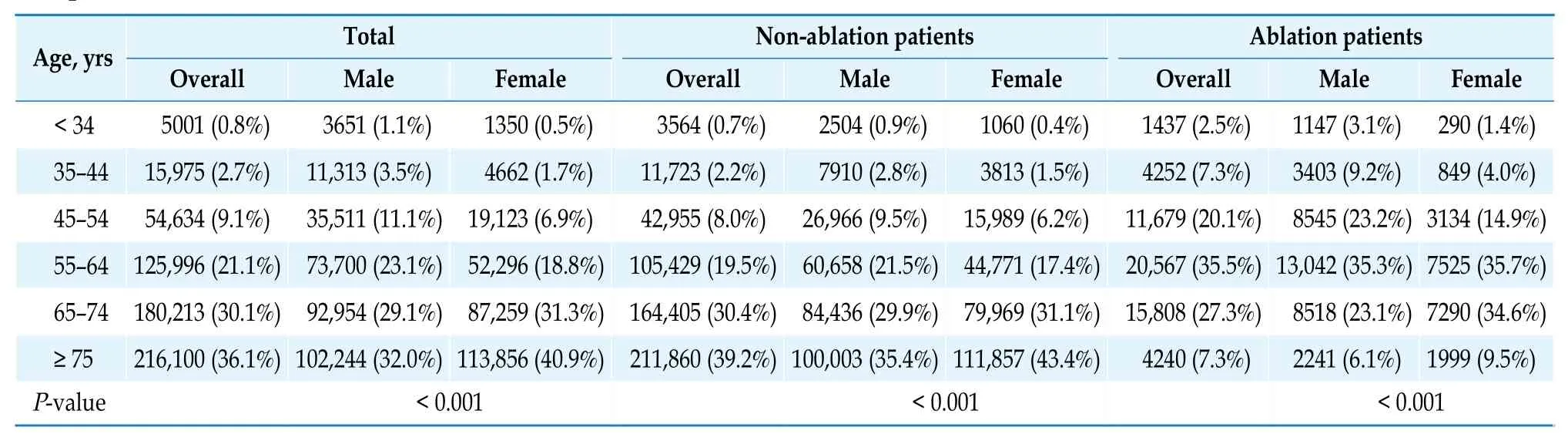
Table 2 Age distribution of all hospitalized patients with atrial fibrillation according to sex and whether or not catheter ablation was performed.
The thrombus score distributions in males and females who underwent catheter ablation also differed(P< 0.001). Furthermore, 71.2% of males had a thrombus risk score of ≤ 1, whereas 59.1% of females had a thrombus risk score of ≤ 2.
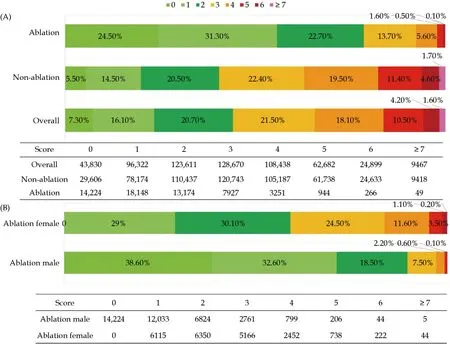
Figure 3 Thrombotic risk score (CHA2DS2VASc) distribution of all hospitalized patients with atrial fibrillation according to sex and whether or not catheter ablation was performed. (A): CHA2DS2VASc score distribution according to whether or not catheter ablation was performed; and (B): CHA2DS2VASc score distribution in the ablation group according to sex.
Comorbidities and Sex Differences
There were fewer associated comorbidities in patients with AF who underwent catheter ablation compared with those who did not. The most common associated comorbidities were hypertension [52.5% overall (47.0% in the catheter ablation group and 53.1%in the non-catheter ablation group),P< 0.001], coronary heart disease [44.4% overall (14.3% in the ablation group and 47.6% in the non-ablation group),P<0.001], HF [39.9% overall (4.7% in the ablation group and 43.6% in the non-ablation group),P< 0.001], and diabetes mellitus [16.6% overall (12.7% in the ablation group and 17.0% in the non-ablation group),P<0.001](Table 1).
In terms of comorbidity, there were differences between male and female AF patients undergoing catheter ablation. Among the AF ablation group, the proportion of female patients with hypertension (51.8%vs.44.2%,P< 0.001), diabetes mellitus (13.9%vs.12.1%,P< 0.001), and HF (5.9%vs.3.9%,P< 0.001) was higher than that of men. There was no significant difference in the proportion of patients with coronary heart disease (14.3%vs.14.3%,P= 0.94), but the old myocardial infarction was more common in males(0.6%vs.1.1%,P< 0.001).
Adverse Events During Hospitalization and Sex Differences
In terms of in-hospital adverse events, 0.2% of all patients experienced pericardial tamponade requiring pericardiocentesis, and 1.2% of all patients experienced all-cause death. The prevalence of allcause death in patients with AF who underwent catheter ablation was lower compared with the nonablation group (0.1%vs.1.3%,P< 0.001). For pericardial effusion/tamponade requiring intervention,the rate in the ablation group was higher than the non-ablation group (0.6%vs.0.1%, respectively;P<0.001) (Table 3). Patients in the non-ablation group sometimes required pericardial drainage due to other clinical conditions, such as chronic HF, hypoalbuminemia, and hypothyroidism. In addition, the incidences of pericardial tamponade requiring pericardiocentesis (0.7%vs.0.5%,P= 0.003) and all-cause mortality (0.1%vs.0.04%,P= 0.006) in females with AF who underwent catheter ablation were higher than in males.
DISCUSSION
Using the HQMS national database of China from 2013 to 2016, we found that catheter ablation for AF increased steadily in China. Patients with AF who underwent catheter ablation were younger, more frequently male, mostly had a lower risk of thrombosis, had fewer comorbidities, and had a lower incidence of adverse events than those who did not undergo catheter ablation. In this population, females were older and had more adverse events than males.
Despite the reported lower age-standardized prevalence of AF in adults (> 35 years) in China (0.7%),the overall burden of AF is very large and is rapidly increasing. Recently, radiofrequency catheter ablation therapy (including AF catheter ablation) has gained traction in China, increasing from 27,000 to 45,000 procedures between 2015 and 2017.[13]Accordingly,the same increasing trend for AF catheter ablation alone was observed from 2013 to 2016 in our study.
We found that most patients who underwent AF catheter ablation had a low-risk thrombotic risk score (males ≤ 1 and females ≤ 2) at tertiary hospitals in China from 2013 to 2016. Worldwide, the risk of thrombosis and stroke in patients with AF who undergo catheter ablation is low. In a single-center study in Michigan, approximately 75% of patients had a CHA2DS2VASc score of 0 or 1.[14]Many studies, but not all, have reported a low stroke rate in patients who have undergone AF catheter ablation. Most of these trials enrolled patients with a CHA2DS2VASc score of < 2, in whom stroke rates will be anticipated to be low.[12]At present, there are still differences between different regions. For thrombotic risk estimation and anticoagulant therapy, regional guidelines should constantly update evidence-based medical evidence, leading to greater benefit for AF patients all over the world.[15-17]
Our data shows that the overall incidence of adverse events was reasonably low in this study. The incidence of pericardial tamponade was 0.6%, and the allcause mortality rate was 0.1% in patients with AF who underwent catheter ablation. Cappato,et al.[18]reported 32 deaths (0.1%) and 331 cases of cardiac tamponade (2.3%) in 45,115 catheter ablation procedures on 32,569 patients with AF at 162 of 546 identified centers worldwide between 1995 and 2006. With advancements in catheter ablation technology, the rates of adverse complications and mortality are decreasing year on year. However, in 2019, Abdur Rehman,et al.[19]reported significant life-threatening complications in 100 patients of 10,378 patients(0.9%). The most common cause was pericardial effusion requiring pericardiocentesis (0.5%) at a sizable quaternary care center between 2000 and 2015.[19]Meanwhile, 1884 complications were identified among 1080 patients (7.2%) in 14,875 cases of AF catheter ablation between 2015 and 2017 in the National Inpatient Sample database.[20]Among the cardiac complications, pericardial effusion predominated (2.18%),followed by cardiac tamponade (1.31%).
In the present study, the incidence of adverse complications is similar to data from a sizable care cen-ter in the United States. Although all patients with AF in our study were from cardiology wards, AF was not necessarily the leading cause of hospitalization.Nevertheless, the incidence of adverse complications in patients with AF who underwent catheter ablation was very low. The possible reasons are as follows: (1) our data were obtained from tertiary hospitals in China, most of which perform more than 100 AF catheter ablation procedures or even more than 1000 AF catheter ablation procedures each year. In addition, most of the hospitals were regional centers; and (2) patients with AF who underwent catheter ablation were younger and had a lower thrombotic risk score than patients who did not, which meant fewer comorbidities and lower overall risk.

Table 3 Incidence of adverse events in all hospitalized patients with atrial fibrillation according to whether or not catheter ablation was performed.
In general, sex differences were identified in age,CHA2DS2VASc score, and adverse events, especially in patients with AF who underwent catheter ablation. The proportion of older patients was significantly higher in the female group than the male group for all patients with AF and subgroups with or without catheter ablation, which is entirely consistent with the trend in Europe and America.[21-24]Numerous national registries have revealed that the pattern of symptoms and management strategies differ between females and males.[25]In a nationwide observational cohort study of 10,135 patients, 42% of patients were female. Women with AF had more symptoms and functional limitations, as well as a lower quality of life, compared with males.[26]Kaiser,et al.[21]also found that in a cohort of 21,091 patients from 2007 to 2011, compared with males, females were older, had a higher CHA2DS2VASc score, and had a higher risk of 30-day hemorrhage and tamponade.A multicenter retrospective study in the United States reported a 5% complication rate in females versus 2.4% complication rate in males (P< 0.001).[27]Kuck,et al.[28]also found that the female sex was associated with a ≥ 36% risk of primary efficacy failure and cardiovascular rehospitalization compared with the male sex. Complication-specific analyses showed statistically significant increases in vascular access complications, cardiac tamponade, pericardial effusion, and postoperative hemorrhage requiring transfusion in females.
Although the reason is unknown, sex-dependent physiological and pathophysiological mechanisms may predispose the female sex to AF later in life. For example, a review of sex differences in those who underwent cardiac ablation procedures suggested that females are referred for catheter ablation less frequently than males, which may play a vital role in the observed age difference.[29,30]In our data, with an increase in age, especially after the age of 65 years, the growth rate in the number of hospitalized patients with AF in the female group was significantly higher than in the male group (Table 2).
LIMITATIONS
There are several limitations in this study that should be noted. Firstly, the institutional representation was insufficient because tertiary hospitals are the highest-level medical institutions in China. Secondly, there was no information on anticoagulant therapy, and the treatment evaluation was not comprehensive. Last but not least, follow-up data after discharge were lacking, so long-term outcome evaluation could not be performed.
CONCLUSIONS
Between 2013 and 2016 in China, most patients with AF who underwent catheter ablation were younger,more frequently male, had a lower risk of thrombosis,had fewer comorbidities, and had a lower incidence of adverse events than those who did not undergo catheter ablation. However, there was a sex difference in the selection of catheter ablation strategies for AF.In the ablation group, females were older and had a higher incidence of adverse events than males. Nevertheless, with progress in AF catheter ablation technology and the accumulation of medical evidence,more patients with AF, especially those at a high risk of thrombosis, will benefit from catheter ablation.
ACKNOWLEDGMENTS
This study was supported by the China-WHO Biennial Collaborative Projects 2016-2017 (No.2016/648722-0). All authors had no conflicts of interest to disclose. The authors thank all China Standard Medical Information Research Centre members for their help and support throughout the study.
 Journal of Geriatric Cardiology2022年4期
Journal of Geriatric Cardiology2022年4期
- Journal of Geriatric Cardiology的其它文章
- Rotor hypothesis in the time chain of atrial fibrillation
- 3D vena contracta area in degenerative mitral regurgitation:cross-platform comparison in a single patient
- New-onset heart failure masking a massive retroperitoneal liposarcoma
- Invasive versus non-invasive hemodynamic monitoring of heart failure patients and their outcomes
- Implication of a novel truncating mutation in titin as a cause of autosomal dominant left ventricular noncompaction
- Tongmai Yangxin Pill combined with metoprolol or metoprolol alone for the treatment of symptomatic premature ventricular complex: a multicenter, randomized, parallel-controlled clinical study