
3D vena contracta area in degenerative mitral regurgitation:cross-platform comparison in a single patient
2022-05-06 08:32:28ShingChingChiuSunYue
Journal of Geriatric Cardiology 2022年4期
Shing Ching, Chiu Sun Yue
Division of Cardiology, Department of Medicine and Geriatrics, United Christian Hospital, Hong Kong, China
Quantification of degenerative mitral regurgitation (MR) by two-dimensional (2D)transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) is challenging. Eccentric, obliquely oriented regurgitant jets limit inter-observer and intra-observer consistency.In recent years, with increasingly sophisticated threedimensional (3D) TTE and TEE systems that enable single-beat 3D color acquisition, 3D vena contracta area (VCA) has emerged as an attractive indicator of MR severity. It overcomes geometric assumptions in 2D techniques and can be acquired in a single cardiac cycle, which is a major benefit in atrial fibrillation. However, most studies of 3D VCA were performed on the Philips TEE platform.[1-3]The performance of the technique on GE systems and on 3D TTE is unexplored. We report 3D VCA measurements in a case of severe degenerative MR on 3D TTE (4V-D transducer, Vivid E95, GE Vingmed Ultrasound,Horten, Norway), and 3D TEE performed on GE(6VT-D transducer, Vivid E95, GE Vingmed Ultrasound, Horten, Norway) and Philips (X7-2t transducer, EPIC 7C, Philips Medical Systems, Andover,MA, USA).
A 73-year-old woman presented with acute dyspnea for two days. She had history of well-controlled hypertension and diabetes mellitus. An apical pansystolic murmur was noted. Chest radiograph showed pulmonary edema. Electrocardiogram showed sinus tachycardia. The 2D TTE (GE)demonstrated normal left ventricular ejection fraction and posterior mitral leaflet flail was performed. Effective regurgitant orifice area (EROA) was 0.8 cm2by proximal isovelocity surface area (PISA)method. Single-beat color Doppler of MR was acquired at apical window on 3D TTE. Image quality was suboptimal at parasternal window. Aliasing velocity was set at default of 66 cm/s. Variance map was turned on to minimize color mosaic on image analysis. Field of view was adjusted to achieve frame rate of 15-20 frames/s. Offline multiplane reformatting of acquired image at peak systole enabled doubleoblique correction of jet orientation and identification of plane perpendicular to jet direction (Figure 1).3D VCA was measured at 1.12 cm2by planimetry of green area on variance map. 3D TEE (Vivid E95, GE)was performed four days later under conscious sedation for preoperative planning. P2 flail due to chordal rupture was confirmed (Figure 2). Singlebeat color Doppler was acquired and postprocessed offline in a similar fashion. 3D VCA was planimetered at 1.21 cm2(Figure 3).
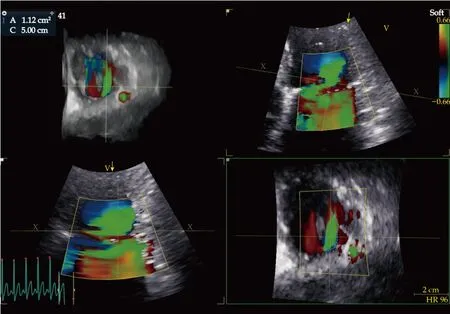
Figure 1 The vena contracta area measures 1.12 cm2 on multiplanar reconstruction of 3D transthoracic echocardiography (Vivid E95, GE) at peak systole. The reconstruction plane is perpendicular to the narrowest neck of color flow on two orthogonal planes, which defines the vena contracta. Aliasing velocity is set at 66 cm/s with variance map enabled.
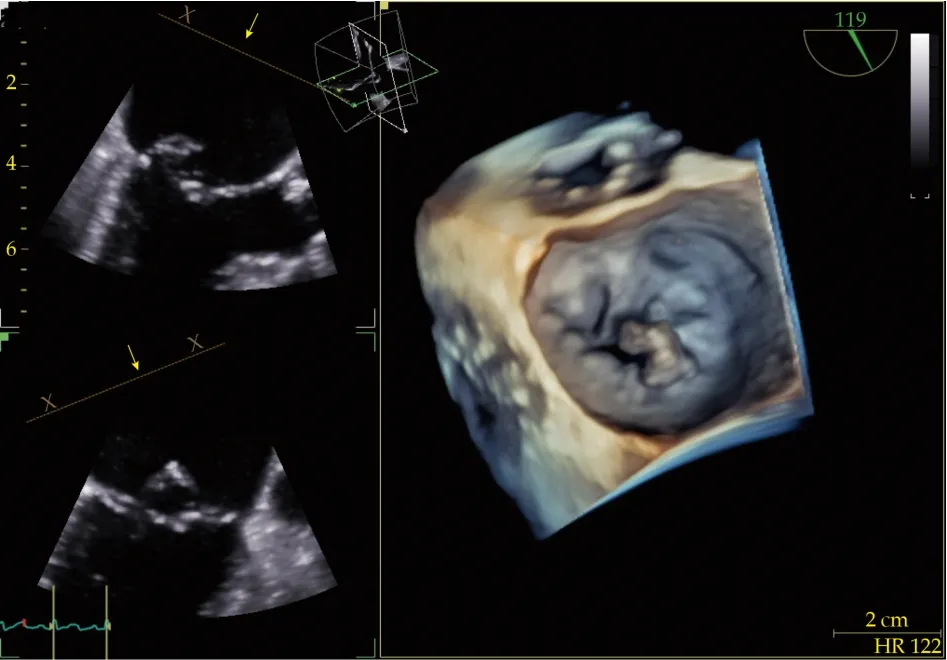
Figure 2 3D transesophageal echocardiography shows P2 segment flail due to ruptured chordae.
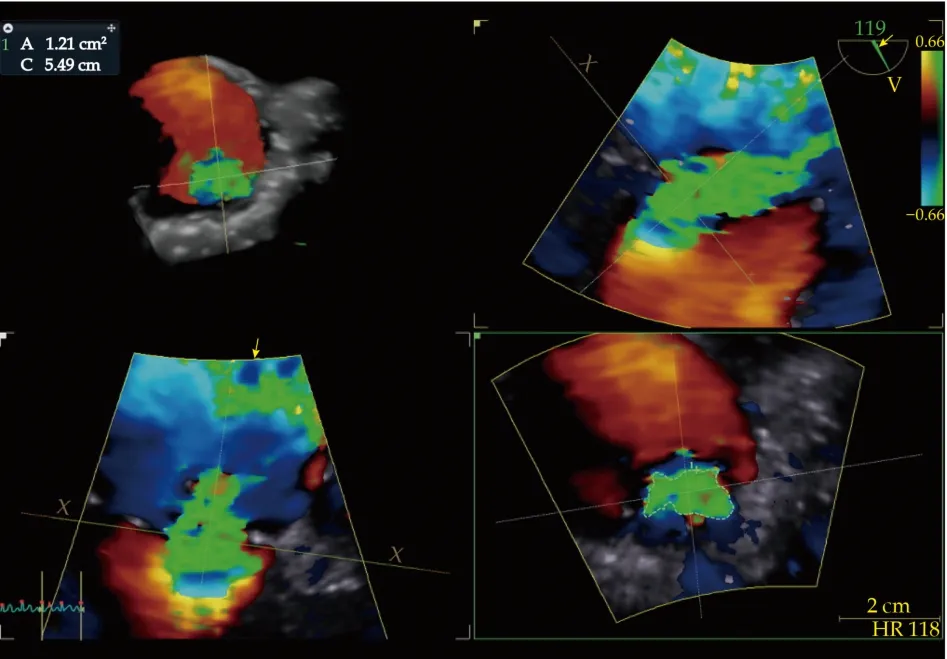
Figure 3 The vena contracta area measures 1.21 cm2 on 3D transesophageal echocardiography (Vivid E95, GE) at peak systole reconstructed in a similar manner as on 3D transthoracic echocardiography.
The patient received open mitral valve repair two weeks after admission during which another 3D TEE(EPIC 7C, Philips) was performed after induction of general anesthesia but before sternotomy. Aliasing velocity was set at 53.9 cm/s; frame rate was adjusted to 15-20 frames/s. Online postprocessing identified a 3D VCA of 1.35 cm2by planimetry of aliased area (Figure 4). Notably, variance map option was not available in 3D color acquisition. Intraoperatively P2 flail and chordal rupture was repaired with triangular resection and mitral annuloplasty leaving minimal MR. The patient remained asymptomatic three months postoperatively.
Our case shows that 3D VCA is highly consistent across platforms (TTEvs.TEE) and vendors (GEvs.Philips), while PISA significantly underestimated EROA compared to 3D VCA. PISA assumes a circular regurgitant orifice, which is rarely the case in eccentric, degenerative MR. For example, the 3D VCA depicts an elliptical regurgitant orifice in this patient. Depending on how the orifice is transected,PISA may underestimate or overestimate the EROA.Several technical details are important to observe in the application of 3D VCA technique. Firstly, singlebeat acquisition is preferred. Stitch artifacts with multi-beat acquisition may distort the color map and introduce error in measurement. Secondly, the field of view should be as small as possible to maximize frame rate, while as large as necessary to include the entire regurgitant orifice. Any truncation of the regurgitant orifice invalidates the result. Last but not the least, aliasing velocity should be set at 55-66 cm/s, which is the default on most systems, and variance map should be turned on if available. We found that higher aliasing velocities deflate the measured VCA, whereas lower values inflate. In addition, speckles of color may intermix at the regurgitant orifice as flow becomes turbulent. It causes confusion to delineation of VCA. Variance map greatly simplifies the situation by dichotomizing the color flow into areas of turbulence and areas without. Turbulence being a hallmark of flow convergence at vena contracta helps to exclude areas of “color blooming”that would otherwise exaggerate the measured VCA.
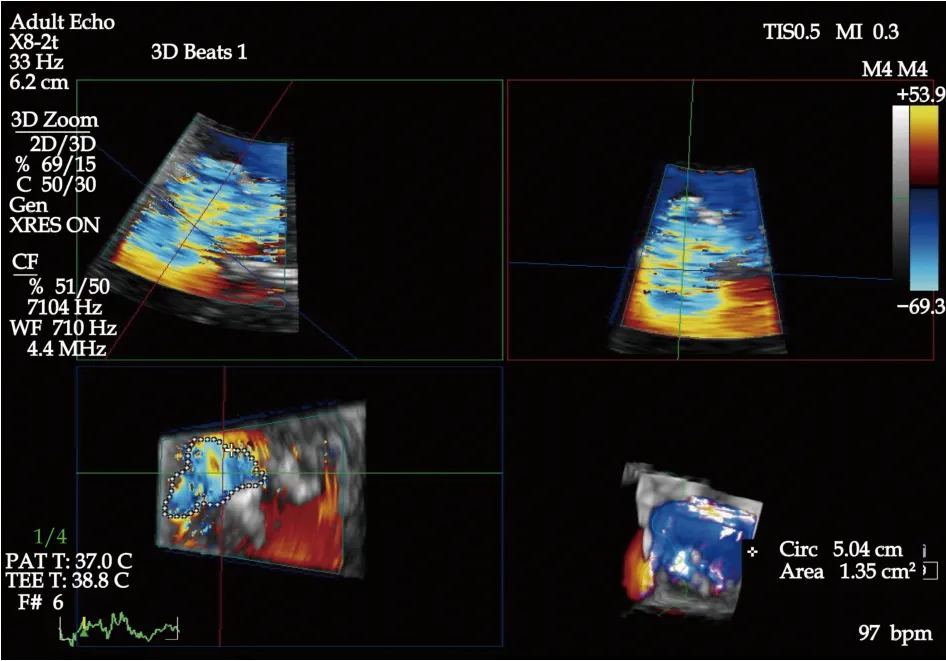
Figure 4 The vena contracta area measures 1.35 cm2 on 3D transesophageal echocardiography (EPIC 7C, Philips) at peak systole. Aliasing velocity is set at 53.9 cm/s. Variance map option was not available in 3D color acquisition on this version of firmware.
In summary, we showed the value of 3D VCA as a feasible, robust measure of degenerative MR across different platforms (TTEvs.TEE) and vendors(GEvs.Philips) in a single patient under different loading conditions ranging from fully conscious to under general anesthesia.
ACKNOWLEDGMENTS
All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2022年4期
Journal of Geriatric Cardiology2022年4期
- Journal of Geriatric Cardiology的其它文章
- Rotor hypothesis in the time chain of atrial fibrillation
- New-onset heart failure masking a massive retroperitoneal liposarcoma
- Invasive versus non-invasive hemodynamic monitoring of heart failure patients and their outcomes
- Implication of a novel truncating mutation in titin as a cause of autosomal dominant left ventricular noncompaction
- Trends and sex differences in atrial fibrillation hospitalization and catheter ablation at tertiary hospitals in China from 2013 to 2016
- Tongmai Yangxin Pill combined with metoprolol or metoprolol alone for the treatment of symptomatic premature ventricular complex: a multicenter, randomized, parallel-controlled clinical study